
Reaching the next level of decarbonization

Being green is something Penn Medicine takes seriously. The hospital system has switched to light-emitting diode (LED) lighting, added variable-speed drives (VSDs) to HVAC equipment when possible, and replaced older chillers and recommissioned entire buildings to increase efficiency, among other things. The system even has entered into a power purchase agreement with a 220-megawatt solar power plant in central Pennsylvania.
All of those efforts are important in the system’s sustainability journey, but Kathleen Fink, energy manager at Penn Medicine, knows that discrete projects that cut emissions and save energy are just the most visible aspects of being green. Today, to be truly focused on sustainability, a health care facility must have a master plan in place, get all hospital departments involved, deal with municipal regulations, and manage downstream and upstream emissions.
All of this boils down to one thing: reducing the hospital’s environmental impact on its community. “It is our hospital’s goal not only to help patients when they come in, but to give them a better environment so they’re less likely to come in,” Fink says. “One of the biggest motivators for making us greener is to help our patients before they even walk in the door.”
Environmental master planning
Developing a plan to improve a hospital’s sustainability seems like a logical step, but most efforts to reduce a hospital’s environmental footprint are ad hoc:
- “Do we need to replace some lightbulbs?” “Well, let’s use LED bulbs this time.”
- “The 30-year-old chiller is breaking down?” “OK, make sure the replacement is as efficient as possible.”
- “We’re building a new facility?” “Great, let’s check out this LEED business.”
Those steps all are good. They save energy and reduce emissions, but having a plan ensures that decisions are always made with sustainability in mind and creates a path toward a diminished environmental impact.
At Penn Medicine, creating a master plan is on the agenda, Fink says. The hospital system’s parent organization, the University of Pennsylvania, has set a goal to become “carbon zero” by 2042, and that goal is driving planning efforts throughout the university. One key step in that direction has been the creation of a new position — director of sustainability — who will coordinate sustainability efforts at all of the hospital’s facilities.

A section of a chilled water system that was part of Penn Medicine’s chiller plant optimization project.
Photo courtesy of Penn Medicine
“The plan is to benchmark and develop a plan for the health system,” Fink says. “One interesting thing is that we have six different main hospitals and several other facilities, and they’re all slightly different. So, everybody’s plan is going to be a little bit different. Some may focus more on energy; some may focus more on environmental. It’s really going to depend on where their weak points are.”
At Mass General Brigham, the health care system that includes Brigham and Women’s Hospital and Massachusetts General Hospital, a strategic energy master plan has been in place for over a decade, and a decarbonization master plan is being developed, says Jason D’Antona, PE, LEED AP, director of engineering and utilities.
“The strategic energy master plan revolves around reducing all utility consumption at our facilities,” D’Antona says. “We are now in the request for proposal stage for a decarbonization master plan, which will come up with a formal plan for us to reduce our carbon emissions, not just through consumption, but also through alternative technologies.”

Mass General Brigham has installed photovoltaic systems at many of its properties, such as this 800-kilowatt array at an affiliate rehabilitation facility in Massachusetts.
Photo Courtesy of Dennis Villanueva, Mass General Brigham Engineering & Utilities Department
The new plan being developed for decarbonization is somewhat being driven by regulatory requirements coming from the state of Massachusetts and local officials, D’Antona says. For example, the Massachusetts Clean Energy and Climate Plan for 2025 and 2030 calls for emissions to be 50% below 1990 emissions by 2030.
“We’ve decided that we need to have a formalized plan that gives us a glide path for our carbon reduction,” D’Antona says.
Emissions source reduction
Naturally, reducing emissions is the biggest part of sustainability. Doing so saves energy and reduces the quantity of greenhouse gas in the atmosphere.
Greenhouse gas emissions are broken into three categories: Scope 1 includes emissions created by the organization, such as from fuel burned on-site to heat a building; Scope 2 is the emissions from purchased electricity, heat and steam; and Scope 3 is emissions external to the organization but directly related, such as emissions from distributed goods used by the organization, business travel and employee commuting.
The first step to reducing emissions often is understanding what the current emissions are, says Andy Woommavovah, CHFM, director of capital project management at Trinity Health, a national Catholic health system based in Livonia, Mich., and a member of the American Society for Health Care Engineering (ASHE) Sustainability Task Force.
“Depending on the size of the organization, staffing levels and expertise, this can be accomplished in-house or with an engaged third party,” Woommavovah says. “Scope 1 and 2 emissions can be more precisely measured than Scope 3. What I have seen is that early performance goals around scopes 1 and 2 can be set and become early wins in the decarbonization journey. Because of the complexity of Scope 3, this category will require a multidisciplinary approach that can include supply chain, investments, safety and security, governance, and social and human capital.”
Generally, controlling scope 1 and 2 emissions are the easiest, says Kara Brooks, LEED AP BD+C, senior associate director of sustainability for ASHE. Controlling Scope 1 emissions can involve projects such as setting back temperatures in unoccupied spaces to reduce natural gas consumption and monitoring leakage of anesthesiology gases. Brooks explains that hospitals enrolled in ASHE’s Energy to Care Program can track Scope 1 energy usage on the Energy to Care Dashboard. Scope 2 emissions come from the utility that provides a hospital’s electricity, steam or heat, and controlling those emissions means reducing the hospital’s consumption of those utilities and/or choosing a utility that generates its energy sustainably.
“I really see health systems and hospitals starting with scopes 1 and 2, because that’s attainable,” Brooks says. “Scope 3 is much more difficult to measure. These are outside the control of the building.”
While most scope 1 and 2 emissions are utility-based and not specific to health care, the Scope 1 emissions associated with anesthesia gases are unique to health care. Brian Chesebro, M.D., medical director for environmental stewardship for the Oregon Region of Providence Health & Services, developed a program to reduce the quantity of leaked anesthesiology gases for his system’s 54 hospitals. Chesebro, an anesthesiologist himself, discovered that many hospitals are leaking from 80% to 98% of their nitrous oxide, a highly potent greenhouse gas.
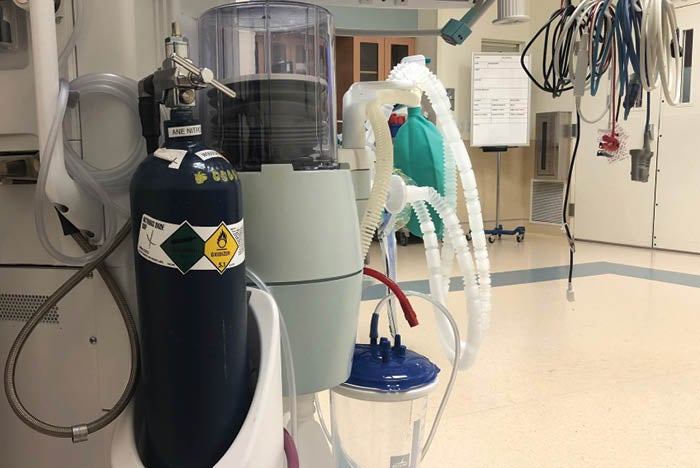
This portable nitrous oxide e-cylinder, which is attached to an anesthesia machine at a Providence Health & Services facility, can be used with 99.7% efficiency versus a central source that is prone to significant leakage.
Photo by Brian Chesebro, M.D.
“The main driver of these nitrous oxide emissions is not the clinical use by the anesthesiologist or [certified registered nurse anesthetist]; the main driver is the integrity of the facility’s infrastructure,” Chesebro says. “For some hospitals, their nitrous oxide-related emissions are greater than the emissions that they generate from burning natural gas for thermal energy. It is surprising for people to learn that a significant portion of their Scope 1 burden is nitrous oxide.”
Chesebro and his colleagues investigated why hospitals were losing so much of their nitrous oxide and identified numerous causes, ranging from supply tanks containing cryogenically frozen liquid nitrous oxide that automatically discharge gas as they heat up to leaky manifolds, and wall outlets and gauges that are not properly attached. In one Providence facility, Chesebro found that a leaky nitrous oxide delivery system was losing 98% of the gas. They switched to using a portable tank system with a closed valve operating strategy and cut the loss to 0.3%.
“That only happened through partnership and collaboration between facilities directors, clinical engineers and anesthesiologists,” Chesebro says. “This work speaks to the value of stewardship being the glue that pulls people together. None of these groups could have figured this out on their own or could have mitigated the source. You need everyone working together to make it happen.”
Every department contributes
In previous decades, sustainability was primarily the province of the facilities department. Because energy consumption is so closely tied to a hospital’s facilities, it makes sense that the facilities department takes the lead on green issues. But it can’t stop there — today, it’s widely understood that reaching green goals requires a whole-hospital effort.
“The facilities department is able to have a major impact on Scope 1 emissions and maybe a limited impact on Scope 2, but the vast majority of scope 2 and 3 emissions are driven by entities outside of the facilities department,” D’Antona says.
The technical phrase for getting everyone involved is “de-siloing.” In other words, the effort is not isolated within the facilities department, but rather spread throughout the organization.
One aspect of de-siloing is understanding that successful large-scale green initiatives need to start with buy-in from the C-suite. Commitment from the top, even if the financial impact of an initiative is not immediately evident, is required for a major effort to succeed.
“As with anything, sustainability initiatives must start at the top,” Woommavovah says. “And at every level below, champions or executive sponsors must be in place to ensure that the program is moving forward in accordance with the schedule.”
Another essential component of de-siloing is getting clinicians on board. Chesebro’s efforts to reduce emissions of anesthesiology gases is a great example of a clinician taking responsibility for a green initiative. Clinicians often are keenly aware of the effects of pollution on patients, especially if they are involved in community health efforts.
Fink says that at her hospital, the physicians have motivated the C-suite to fully embrace the green efforts.
“Part of the push to our corporate C-suite has been from the physicians themselves,” she says. “They’re extremely motivated.”
Getting the rest of the hospital on board may start with small efforts. People working in the food service department, for example, can take ownership of increasing the percentage of recyclable materials that end up in the recycling receptacle. And people in the administrative office can take the bus to work instead of driving, which can help a hospital reach its Scope 3 emissions goals.
“When you add them all up, these activities are going to make a big difference,” Brooks says. “Low-cost and no-cost measures can be very impactful. For one thing, even doing something small like that helps give ownership and empowers people to do more.
“That’s why we say just get started. Just shut off your lights or shut things down, or cut back your temperatures when your space is unoccupied,” Brooks says. “It may not make a huge difference right away, but it starts to create some culture and behavior change. You absolutely have to have that culture shift within your entire organization to really make a big difference.”
More examples
There are countless ways to reduce a hospital’s environmental footprint. Besides those mentioned above, here are a few more examples:
- Optimize chillers. Penn Medicine hired a firm that examines the entire chilled water system to ensure everything is running as efficiently as possible. At one of the Penn Medicine hospitals, that effort alone reduced the hospital’s electricity consumption by 25%.
- Consider alternative energy sources. Mass General Brigham is building several ambulatory care facilities that will use ground source heat pumps for temperature control. Ground source heat pumps take advantage of the constant temperature of the ground to efficiently provide heating and cooling. The system also is installing photovoltaic panels on the roofs of their parking garages to offset electrical consumption.
- Use building automation systems. Most modern hospital facilities have building automation systems that can control lighting, HVAC and other energy-consuming equipment. But many are out of date or poorly calibrated; fixing those can help a facility reach its green goals.
A complete effort
The journey to a more decarbonized health care system includes much more than upgrading the lighting or turning down the heat. A complete effort is required to truly become a green organization.
“You must have top-level leadership support and involvement; understand your footprint; set goals; develop a sustainable plan that is scalable to the size of the organization; manage your data and ensure that it is all-inclusive and all agree to it,” Woommavovah says. “Do not start without having these critical pieces identified.”
Related Articles

Satisfaction rates improve with new proactive approach
Rural hospital's switch preventive maintenance eases work order volume and anticipate future challenges..

Helping health care facilities do less with less
The guiding strategy and evolution of a market-leading health care CMMS.

Results of the 2024 Hospital Operations Survey
Maintenance teams align their resources and responsibilities despite labor and budget shortfalls.