
New ASHRAE standard for hospital water systems

The new standard calls for a designated multidisciplinary team to ensure the program is effective and implemented as designed.
Image by Getty Images
The Centers for Medicare & Medicaid Services (CMS) on June 2, 2017, issued its S&C Letter 17-30, which “expects” CMS-certified facilities to have water management policies and procedures to reduce the risk of Legionella and other opportunistic pathogens in building water systems. Among the resources CMS recommended in developing such programs is the American National Standards Institute (ANSI)/ASHRAE Standard 188, Legionellosis: Risk Management for Building Water Systems.
This was followed on June 24, 2021, by the Centers for Disease Control and Prevention (CDC) publishing a Legionella toolkit called “Developing a Water Management Program to Reduce Legionella Growth & Spread in Buildings,” which also referenced Standard 188. The toolkit recommends steps to identify at-risk buildings, build a water management program, create a designated water management team, identify potential areas where Legionella could grow and spread, create control measures and corrective actions, and monitor corrective measures.
Most recently, ASHRAE introduced ANSI/ASHRAE Standard 514, Risk Management for Building Water Systems: Physical, Chemical, and Microbial Hazards. According to ASHRAE, “Standard 514 pulls back to address microbial risk more broadly, and the associated physical and chemical hazards associated with its mitigation.” A logical extension of ASHRAE’s previous efforts, ASHRAE 514 provides a new tool to help hospitals improve their water management programs.
The ASHRAE standards can be accessed online.
Potential impact
Implementation of ASHRAE 514 in health care facilities would require changes on several levels. Not only is compliance with ASHRAE 188 a requirement of ASHRAE 514, but it also adds specific requirements to address multiple hazards. The standard further adds a higher level of sophistication to the water management program.
Implementation would involve more people to manage the program. Plan development would require additional time and information supplied from various departments to tailor the plan to the facility. In addition to the facilities department, the designated water management team would include nursing, infection preventionists, contractors, consultants, epidemiologists and environment of care (EC) leaders to ensure the program is effective and being implemented as designed. Moreover, a successful plan would require ongoing communication between these departments.
Because preventive maintenance or repairs of the domestic water system would have specific guidelines to keep any contaminants from entering potable water systems, operations would also change.
Disinfection and flushing will likely occur more frequently due to repairs or alterations. If determined by the designated team, monitoring of incoming potable water for disinfectant levels, chemical contamination, pH, conductivity and temperature would need to be consistent. Domestic hot water temperature would also need to be controlled to prevent scalding. Additional documentation of the system operations may be necessary.
Implementation would affect the way health care facilities manage construction projects. It would no longer be left exclusively to the engineer to design a potable water system and the contractor to install it. There will need to be collaboration with members of the designated team in the design phase to ensure a compliant potable water system.
A building block
The current water management program provided in ASHRAE 188 is a foundational building block for ASHRAE 514. Most of the elements are similar; however, the requirements are more developed in ASHRAE 514. There are seven elements of a water management program under ASHRAE 514. A brief overview of each element includes:
1. Establish a designated water management team. ASHRAE 188 lays out the foundation for a basic water management team. It consists of building owners or individuals who are familiar with the building’s water system and have knowledge of the system’s design and water management as related to legionellosis. ASHRAE 514 states that the designated team shall include but not be limited to:
- One or more of the building owners or their designees, employees, suppliers, contractors, consultants or building water systems design professionals.
- A building owner or senior leader who can make command decisions.
- A member of the facilities management staff with knowledge of building water systems.
- An individual who has knowledge of the health care facility’s infection prevention and control program.
- An individual responsible for clinical care leadership at the health care facility.
- A member of occupational and environmental safety (OES) management if the facility has an OES program, or a member of EC management if the facility has an EC program.
ASHRAE 514 is more prescriptive in the selection of the individuals to serve on the designated team to make it robust and effective in implementing and overseeing the water management plan.
2. Describe water systems/flow diagrams. ASHRAE 188 requires a graphical depiction of the water system to be described in step-by-step process flow diagrams. The diagrams shall have detail that enables the identification, analysis and management of the risk of legionellosis throughout the building water systems. The diagram describes how water is processed and delivered to endpoint users and gives the location of water processing and components. It also indicates how water is received and processed.
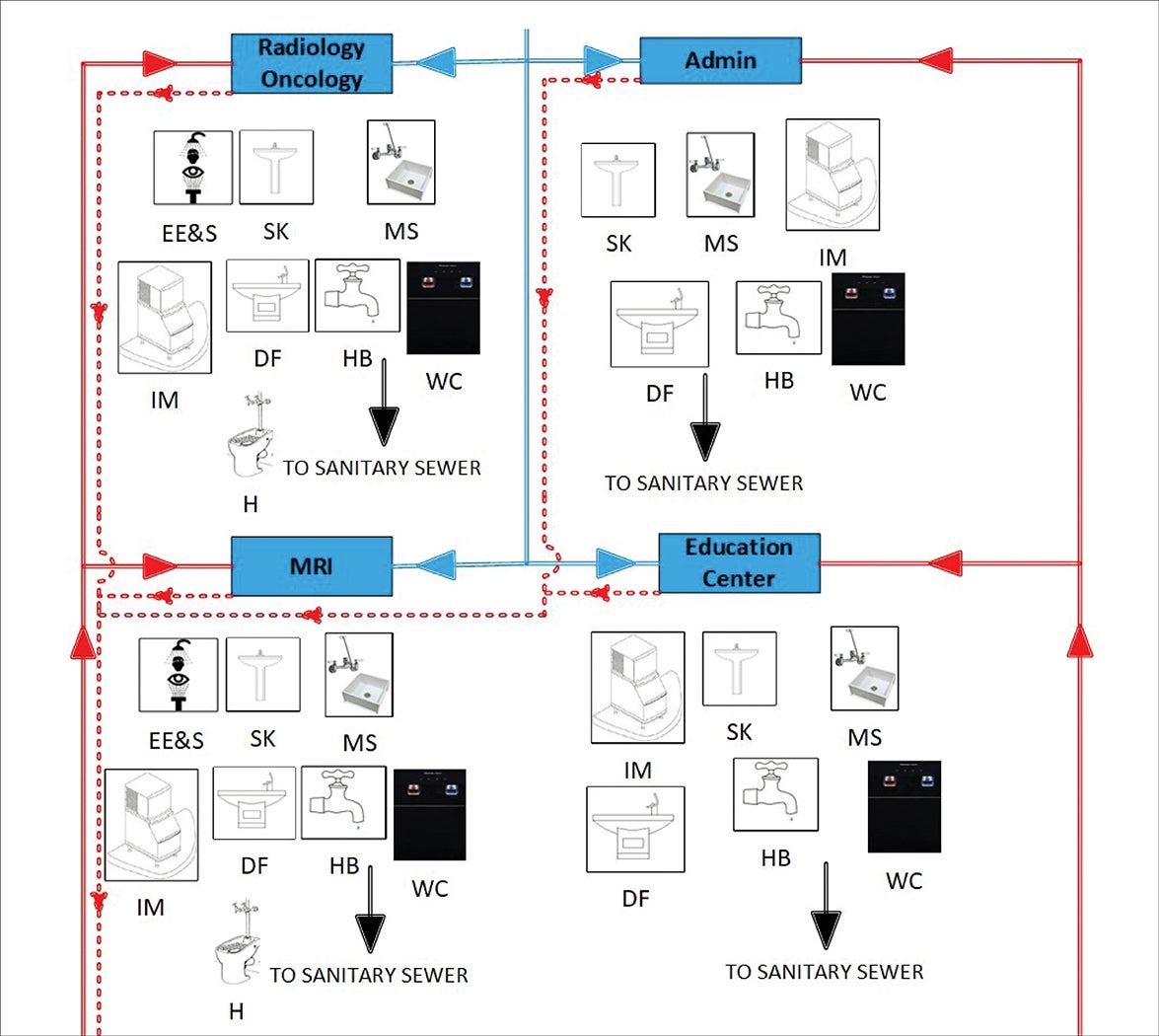
Click image to expand
ASHRAE 514 has the same language but adds other requirements to the water system description and process flow diagrams, including:
- Identifying the type of disinfectant(s) in the water supply entering the building.
- dentifying potable or connectable medical devices that can expose patients or occupants through medical use.
- Describing “high risk areas where hazardous conditions in the building water systems could have the potential to contribute to the risk of physical, chemical or biological hazards, such as that contribute to risk of illness or injury from physical, chemical, and microbial hazards, including clinical areas, dietary areas, central sterile support areas, patient care areas, and other high-risk areas.”
- Other areas as deemed appropriate by the designated team.
The building flow diagrams will need to be more sophisticated, identifying all water use points, including sterilizers, scope washers, central dialysis systems, eyewash stations and any connectable medical device that could expose patients to the water from the building water system through their medical use. Under ASHRAE 514, health care facilities will not only monitor microbiological risks but also physical and chemical hazards.
3. Analysis of building water systems. ASHRAE 188 requires a graphical process flow diagram be used to evaluate where potentially hazardous conditions could occur in the system and where control measures are to be applied to potentially hazardous conditions. This also includes an assessment of risk to vulnerable building occupants that could be exposed to the building water system. In addition, the consequences of water outages will need to be assessed. This primarily addresses cooling towers; heating, ventilating and air conditioning equipment; whirlpools and spas; and other elements. ASHRAE 514 has added physical and chemical risks, high-risk areas and high-risk clinical areas that are now included on the building flow diagram.
4. Control measures. Both ASHRAE 188 and ASHRAE 514 require the designated team to determine what control measures to implement based on the analysis. These include all processes, procedures and activities or actions to maintain the physical or chemical conditions of water within established control limits. The control measures will be determined by the designated team, which will identify the minimum and maximum values and ranges for the chemical and physical parameters of each control measure.
5. Monitoring/corrective actions. The designated team establishes a monitoring procedure to determine whether the control measures are within the specified limits. The team also determines how and when control measures are implemented.
ASHRAE 514 adds physical and chemical language to the standard. The designated team establishes the corrective action to be taken when monitoring determines that the measured parameters fall outside of their values and ranges. The team will decide who implements the corrective actions and notification processes.
6. Confirmation. ASHRAE 188 and ASHRAE 514 have similar language for confirming water management program effectiveness. However, ASHRAE 514 adds the physical and chemical parameters to the control measures. The language also shifts to validation rather than confirmation. The validation process includes:
- Measuring the physical and chemical parameters at representative points throughout the water system to determine whether the values and ranges are within limits. The designated team will determine the frequency, collection procedures and test methods that are used to validate the program.
- Clinical surveillance for infection from waterborne biological hazards.
Additionally, if it is determined that biological testing should be performed, part of the determination to test for microbiological hazards should be based on:
- Evidence that control measures for microbiological hazards in the water system are not being maintained within control limits, including the water systems that have supplemental disinfection.
- Whether there are at-risk or immunocompromised patient populations in the facility.
- Whether there is a history of illness associated with building water systems in the facility.
7. Documentation and Communication. Additional requirements of ASHRAE 514 are implementation, documentation and communication procedures for:
- All activities of the water management program.
- Coordination with those covering different portions of the building water system and associated equipment.
- Informing all affected parties identified by the program of changes.
- Maintaining and documenting revisions that replace earlier versions of the water management program.
- Notification of the designated team when illness or injury caused by physical, chemical or microbial hazards associated with the building water system is suspected or identified to be epidemiologically linked to the health care facility.
- Informing all affected parties identified by the program of actions taken when the designated team determines there is elevated risk of injury, illness or disease caused by building water system physical, chemical or microbial hazards.
Other requirements. Under Section 8, Requirements for Health Care Facilities, there are also requirements for the designated team to review new construction and any revisions, and assess the risks associated with the project to adjust the risk management plan. This is to be accomplished in the early planning stages, during each phase of design and construction and at startup of the building water system.
ASHRAE 514 also requires health care facilities to adhere to ASHRAE 188. Some of the additional requirements are:
- Documented procedures for disinfection and flushing before occupancy.
- Documented procedures for recovering from an operating outage or failure of water treatment as well as repairs or component replacement.
- Documented procedures based on manufacturers’ instructions for maintenance or cleaning of system components.
- Documented procedures for restoring operations after a water interruption or water supply piping break.
- Documented identification of persons responsible for water treatment and applying water treatment products.
- A contingency response plan for potable hot and cold water to address water sampling and locations, test methods in response to disease or outbreak as well as the corrective action plan and the persons responsible.
Comprehensive approach
In 2021, there were 52 waterborne disease outbreaks in the United States, according to the CDC. Also, at least 45% of the nation’s tap water could be contaminated with at least one form of PFAS, known as “forever chemicals,” according to the U.S. Geological Survey.
In health care, many patients could be immunocompromised or highly susceptible to many of the chemicals and organisms in drinking water. The normative and informative references in ASHRAE 514 give an idea of the hazards.
ASHRAE 514 provides a comprehensive approach to managing hospital water systems for the benefit of patients, families and staff.
RELATED ARTICLE: Building a water management team
Developing a designated water management team and keeping information flowing to all appropriate parties can be a daunting task for a single health care facility, and even more difficult for a large health care system. The following suggestions may help in this endeavor:
- Choose a leader. Facilities managers should pick a leader who is good at organizing and keeping on task. They should be good at taking notes and assigning tasks for the other team members to complete. The leader could also be the person who creates the written version of policies and procedures to be discussed at future meetings.
- Choose the right people. It is always important to have the right people. The designated team will need to be diverse with clinical and water management knowledge. Facilities managers should pick the subject matter experts in their field who have worked on policies, are seasoned leaders and who can positively contribute to the team.
- Be consistent. Facilities managers should be consistent with meeting times and days. They should try to pick a date and time convenient to most.
- Use technology. COVID-19 caused many health care organizations to switch to web-based systems for communication. This has become a great way to conduct business meetings and will likely continue. Web-based folders that team members can access would make it easy to share information with each other.
- Verify and validate. Facilities managers should review the water management program for alignment with the current standards and address gaps. Confirmation is an essential component of the program.
Many health care facilities managers are likely using some or all of these suggestions, especially if they are in a large health care setting spread out over multiple campuses. The point is to leverage everything available to have a highly successful designated water management team.
James “Craig” Ayers, MHA, CHFM, CHC, CHSP, CSMP, CPO, SASHE, is director of system engineering services at Memorial Hermann Southeast and Pearland hospitals in Houston. He can be reached at james.ayers@memorialhermann.org.
Related Articles

NFPA weekly update: March 2-6
The latest updates on codes and standards for sprinkler system installation, fire alarm and signaling devices, and emergency communication systems.

NFPA weekly update: Feb. 23-27
Codes and standards on fire doors, emergency power systems and building construction safety codes move to the next stage.

NFPA weekly update: Feb. 16-20
The 2027 editions of NFPA's Life Safety Code and Health Care Facilities Code are open for the motioning process.