
Boosting sustainability through electrification

Providence St. Peter Hospital in Olympia, Wash., was selected for a groundbreaking feasibility study.
Image courtesy of Providence St. Peter Hospital
Recognizing the growing interest in decarbonizing the health care sector, the American Society for Health Care Engineering (ASHE) sought to support its members wishing to decarbonize their facilities.
There had been extensive effort on guidance for decarbonizing new hospital buildings, but little information was available about the decarbonization of an existing hospital building. Additionally, there was speculation about the feasibility of decarbonizing an existing hospital from a technical and financial perspective.
In April 2023, ASHE explored the concept of sponsoring a comprehensive case study investigating the feasibility of decarbonizing an existing hospital building with Providence, a not-for-profit health system serving the western United States. Providence was identified as a key partner due to its leadership in environmental sustainability and its desire to share lessons learned with the field.
The resulting 180-page case study, titled Electrifying Heat in an Existing Hospital: Providence St. Peter Hospital Decarbonization Case Study, from which this article was excerpted and edited.
Selecting a hospital
The push toward decarbonizing health care facilities has been underway for several years. However, concerns have lingered about the feasibility of achieving this within the existing facility stock.
This concern is especially true for Scope 1 emissions or combustion that takes place on-site. On-site combustion primarily serves heating systems, which account for approximately 90% of Scope 1 emissions. The health care design, construction and operations community has proven it is possible to develop a new health care facility that achieves Scope 1 carbon neutrality and, if only renewable electricity is purchased, Scope 2 carbon neutrality.

Numerous resources exist such as the ASHRAE/ASHE Decarbonizing Hospital Buildings guidebook for new hospitals. The question ASHE wanted to answer with Providence was, “Can we cost-effectively decarbonize an existing ‘typical’ hospital?”
A significant factor to consider for decarbonization is the embodied carbon of existing hospitals. Replacing older hospitals with new ones designed to operate at net zero carbon requires significant construction materials and generates demolition waste, all of which emit carbon in their production, transportation and disposal.
The Providence team and ASHE selected Providence St. Peter Hospital (PSPH), a 733,000-square-foot, 372-licensed bed community hospital in Olympia, Wash., for the study. It is a typical large inpatient hospital that represents a reasonable reference for the health care field. The operations and unique features of hospitals, such as requiring steam for sterilization, make them more complex to electrify than many other commercial buildings.
The facility was originally constructed in 1968 and has included several additions since it opened. It has a variety of envelope and heating, ventilating and air-conditioning (HVAC) systems in place, and the heating system is served by a central steam boiler plant.
The hospital was already efficient, operating with an energy use intensity (EUI) between 200 and 205 kilo British thermal units (kBtu) per square foot per year. For reference, ASHE’s Energy Benchmarking for US Hospitals report indicates that the average EUI is approximately 228 kBtu per square foot per year.
Geographical location and climate also were considered when selecting a case study hospital, and the mild climate of Olympia was considered appropriate because it represents a baseline case study demonstrating the feasibility of decarbonizing in a temperate geographical location.
The fact that PSPH was ahead of many others on its journey toward decarbonization also was considered. The hospital has robust utility and building metering and utilizes 100% renewable power.
As a health care system, Providence has developed a climate action plan that incorporates decarbonization strategies for anesthetic gases, transportation, waste and electricity. For PSPH, the missing piece from the overall decarbonization strategy was the thermal energy load. For that reason, the ASHE study investigated decarbonizing the thermal load specifically. PSPH also has a data collection system that can inform a decarbonization study.
ASHE and Providence agreed to conduct this decarbonization study to help facilities develop their own site-specific Scope 1 decarbonization plans, in keeping with their own organizational carbon reduction goals and to access the technical, operational and cost feasibility of Scope 1 decarbonization in light of unfolding and accelerating laws requiring building decarbonization.
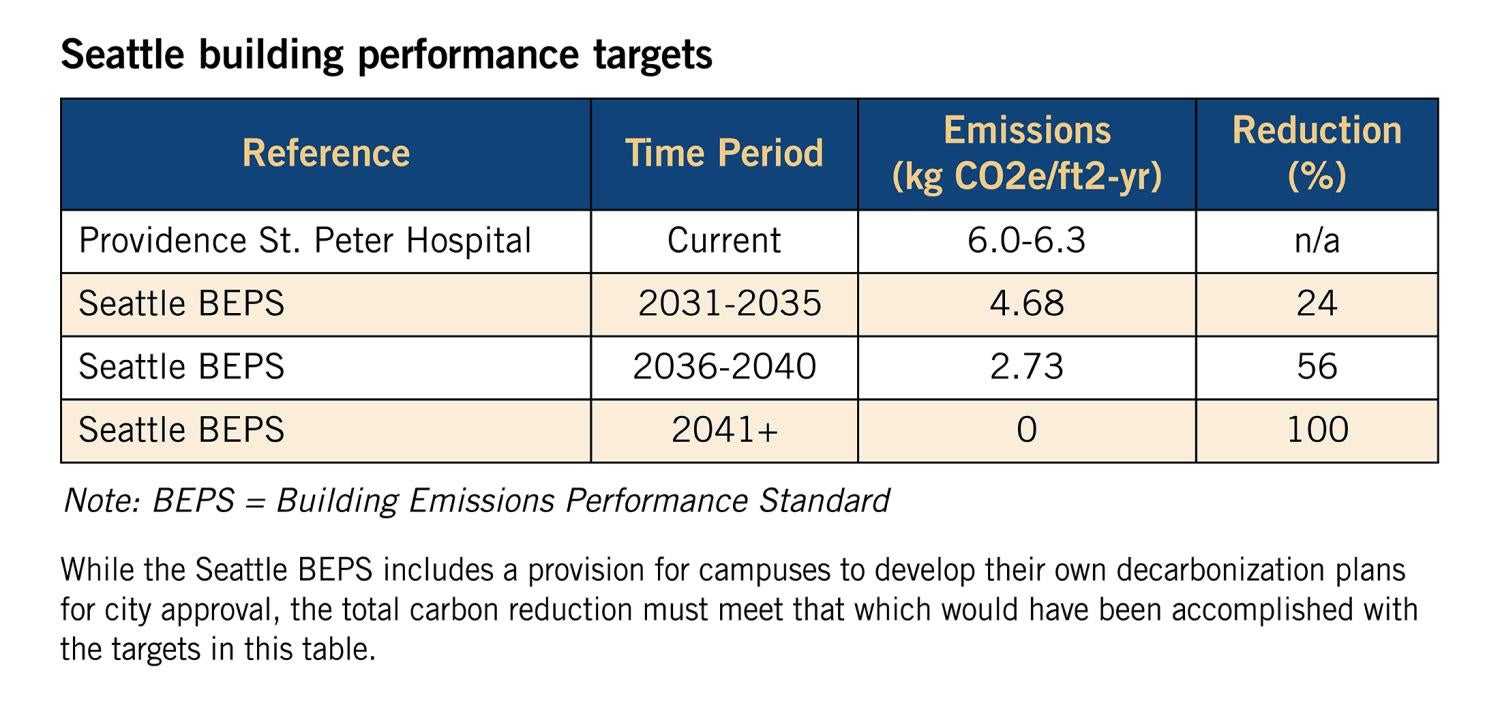
The city of Seattle, which is located approximately 1 1/2 hours away from PSPH, passed one such law, the Building Emissions Performance Standard (BEPS) in 2023, with specific rules set for adoption in 2024. The Seattle ordinance is the basis for this study’s assessment of decarbonization timing and estimate of potential fines for failure to comply with the regulation. While the Seattle BEPS includes a provision for campuses to develop their own decarbonization plans for city approval, the total carbon reduction must meet that which would have been accomplished under the targets.
Major challenges
Two major challenges addressed in the study are determining pathways to achieve electrification of the health care facility’s heating plant while maintaining a resilient supply of energy and supporting a full service of operations, and determining the impact on the electrical utility supply to achieve beneficial electrification.
The goal for PSPH is to eliminate combustion-based Scope 1 emissions by electrifying the heating plant that currently exists, consisting of two dual-fueled boilers. This goal also includes discontinuing the natural gas supply to eliminate the associated upstream methane leaks and complements the 100% renewable electricity already being purchased by the hospital.
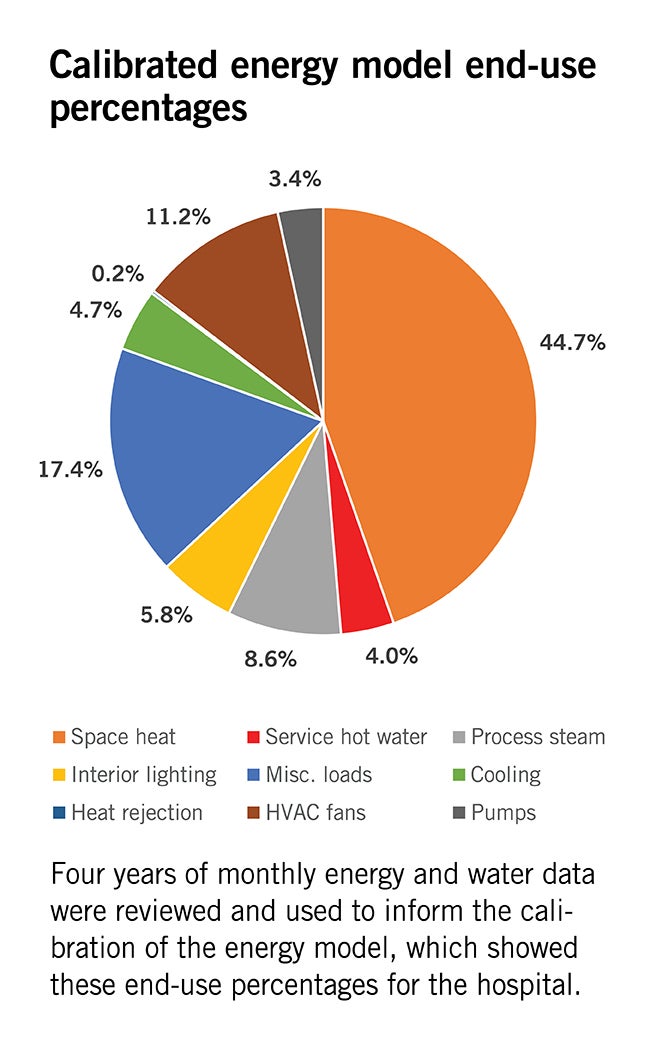
The approach to assessing and decarbonizing PSPH was to carefully analyze the existing conditions, energy use and peak heating demand by end-use. The next step was to identify approaches to reduce heating loads through investments in certain technologies and account for the overall impact. A calibrated energy model was developed per ASHRAE Guideline 14, Measurement of Energy, Demand, and Water Savings, requirements to fill in any data gaps and to further support energy and financial analyses.
Click image to expand
The recommended strategy is based on a systems-thinking approach to address as many demand-side energy-saving measures as feasible to reduce the plant load. The installed heating capacity is 25 million British thermal units (Btu) per hour (MMBtu/h) (7,327 kilowatts (kW)), and the measured peak load is 20 MMBtu/h (5,861 kW), which can be reduced to 11 MMBtu/h (3,224 kW) if all demand-side measures are implemented.
The reduced heating load will enable greater flexibility on the heating hot water (HHW) distribution side in terms of smaller pipe sizes and lower temperatures. The target peak HHW temperature is 140 F to achieve efficient heat pump operation. However, this depends on the level of implementation of demand-side measures, especially on the envelope upgrades.
Upon completion of the distribution system upgrades, the heating plant can be upgraded with air-source heat pumps as the primary source of thermal energy for normal operation and augmented with a heat recovery chiller and 100,000 gallons of HHW storage.
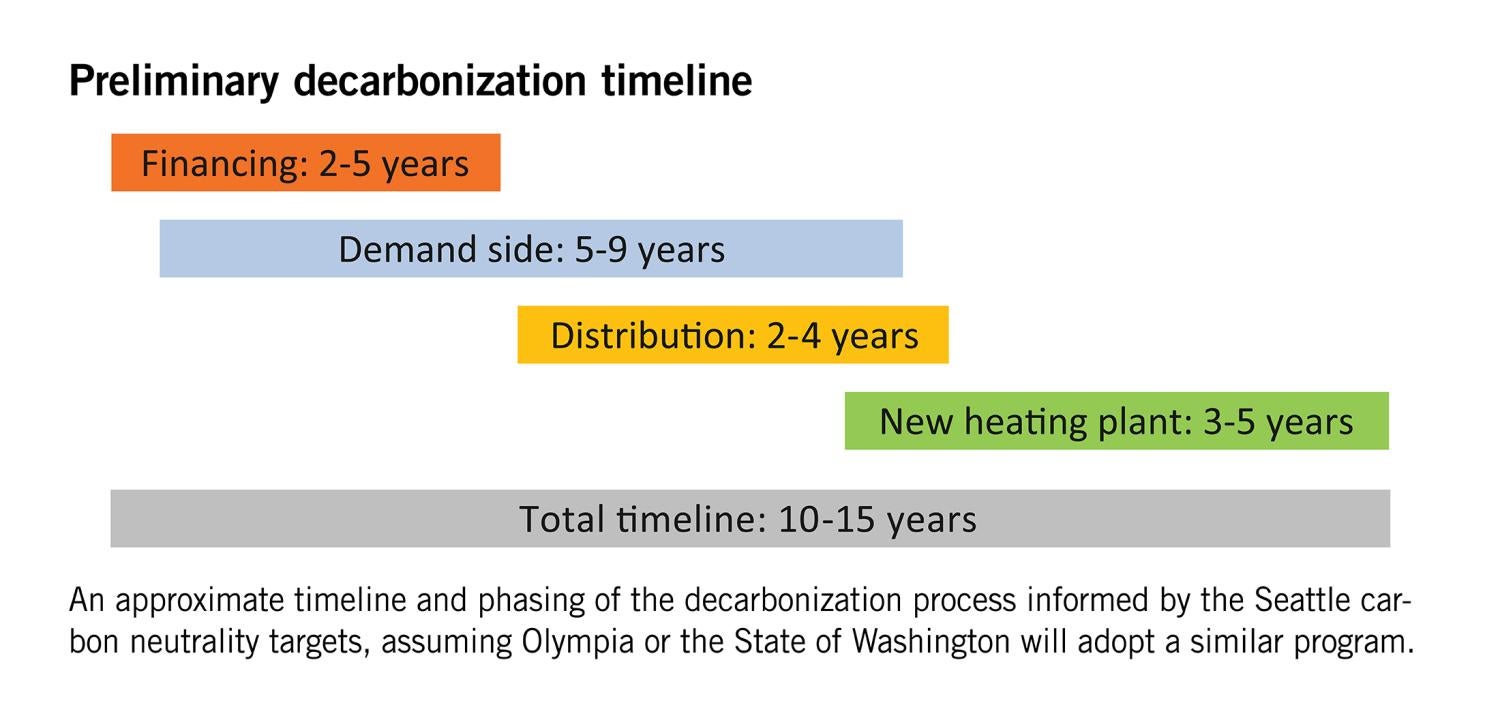
The implementation of the decarbonization strategy will need to be phased and may take several years to implement, depending on available resources. The recommended phasing is as follows:
- Demand-side upgrades (nine-year duration), such as implementing air-side heat recovery upgrades; adding insulation and glazing upgrades; upgrading process steam-using systems (kitchen and sterile processing areas); and continuing to implement other energy-saving measures.
- Distribution system upgrades (one- to two-year duration), such as migrating loads to existing HHW pipes after demand-side upgrades are completed and replacing steam pipes with HHW pipes (starting in spring to have seven months of low heating demand before cold weather arrives).
- Replacing steam converters with heat exchangers for service hot water loops and adding a variable primary HHW pumping system.
- Plant system upgrades (three- to five-year duration), such as adding a south expansion or penthouse to the central utility plant to house the air-source heat pumps; upgrading electrical infrastructure and adding generators and generator jacket heat recovery; installing air-source heat pumps; decommissioning boilers; and installing thermal storage or microgrid in boiler footprints.
Click image to expand
There are two somewhat unique features at PSPH that simplify the electrification and decarbonization process.
First, the hospital does not have humidification because the marine climate does not require it. Relative humidity data was analyzed that demonstrated compliance with a minimum 30% relative humidity for all hours, with excursions below 30% for less than 12 hours per year. The relative humidity did not fall below 20%.
Second, the service hot water (SHW) system operates at 120 F, which simplifies serving the SHW from the HHW loop rather than either running a warmer HHW loop or applying a stand-alone heat pump system. Although it is more common to operate SHW systems at 140 F per Centers for Disease Control and Prevention guidance, no Legionella concerns have arisen at PSPH because of the lower temperatures.
The resilience strategy is to maintain on-site diesel fuel storage that can support generators and boilers in the near term. The generators will be upgraded to include engine jacket water heat recovery to support the heating demand during a power outage when the plant is upgraded. The heat recovery effectively turns the generators into a combined heat and power system providing both electrical and thermal energy to the hospital during outages. The boilers will stay in place until operational proficiency is achieved with the heat pump plant and generator heat recovery.
Current testing and emergency power use accounts for approximately 4% of annual on-site combustion emissions. Resilience solutions, such as thermal storage and microgrids, will be reevaluated to replace the boilers as the technology matures.
Microgrids are being implemented in a few hospitals today that can be referenced for this study and should align with this project’s timeline. For now, on-site fuel storage is being accepted as a resilience solution because it is a small emission source due to few run hours and it assists in eliminating the natural gas connection that results in methane leaks.
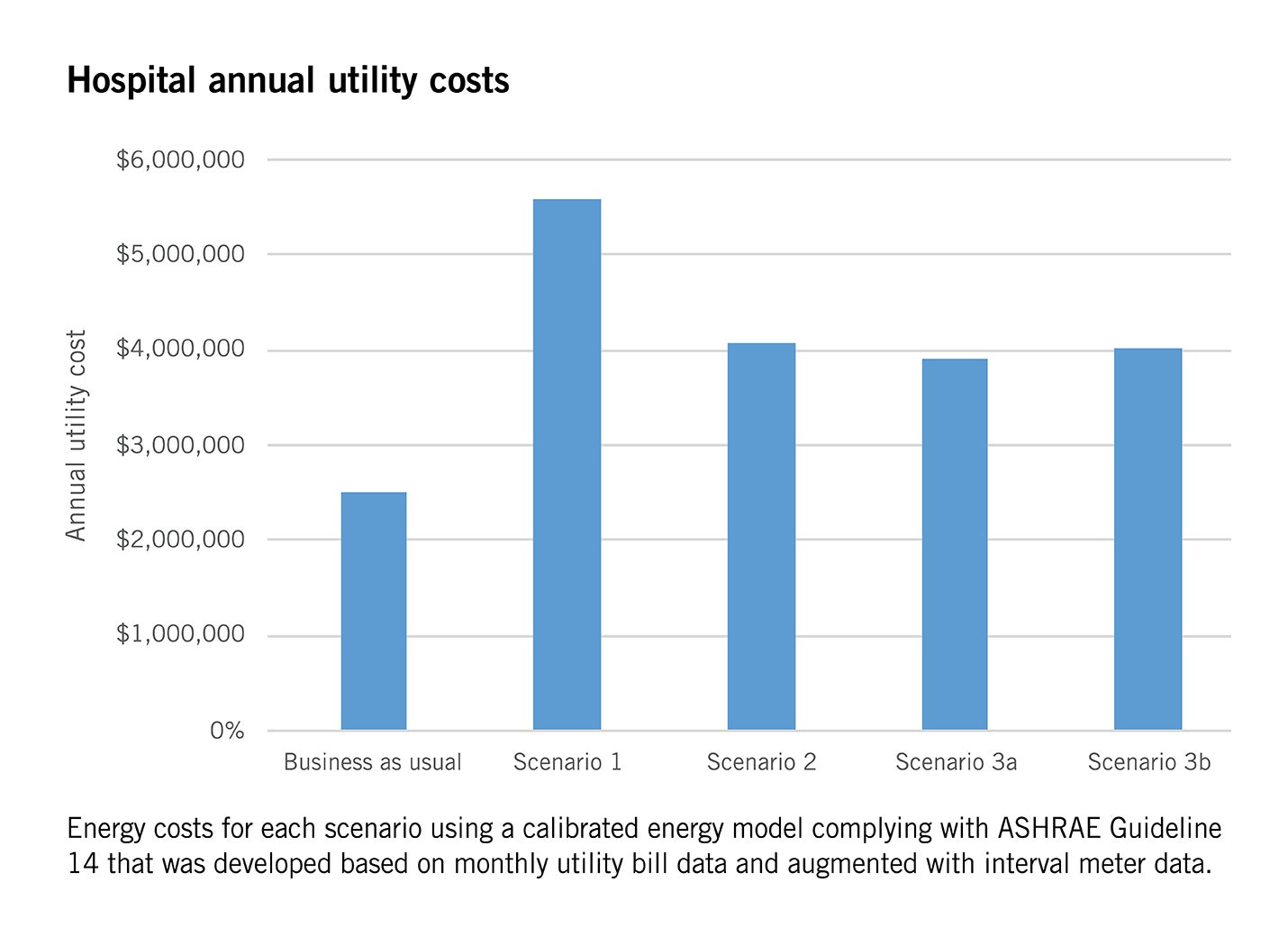
The study investigated four potential scenarios for the hospital between 2024 and 2041 based on a regulatory framework of the Seattle BEPS.
- Scenario 0 is a business-as-usual case where the hospital accepts a one-time $7.5 million fine and makes incremental capital improvements over time.
- Scenario 1 is the minimum disruption scenario that only replaces the existing dual-fuel boilers with two electric resistance boilers plus supporting generators and leaves the balance of the systems in place.
- Scenario 2 implements demand-side energy-saving measures on 100% outside air systems, electrified process loads with heat pumps or stand-alone electric boilers and a host of other demand-side energy-
saving measures. An air-source heat pump plant would then be implemented to support the 16 MMBtu/h (4,689 kW) heating load. - Scenario 3A adds envelope energy-
saving measures to replace single-pane windows and insulation to uninsulated or partially insulated walls. The envelope measures reduce the heating load to 11 MMBtu/h (3,224 kW). - Scenario 3B was broken out to isolate the impact of the insulation improvements because it is a costly upgrade with a poor return on investment.
Click image to expand
A third-party cost estimate was developed to inform the three decarbonization scenarios. The capital cost for Scenario 1 was estimated to be $57,711,000, or $79 per square foot; Scenario 2 was estimated to be $62,171,000, or $85 per square foot; Scenario 3A was estimated to be $80,425,000, or $110 per square foot; and Scenario 3B was estimated to be $68,400,000, or $93 per square foot. For reference, a full tenant improvement (TI) on a hospital is between $100 and $150 per square foot. However, the square footage is the entirety of the hospital, or 733,000 square feet. Also, the TI is nearly exclusively focused on infrastructure enhancements, which is atypical for a TI.
Click image to expand
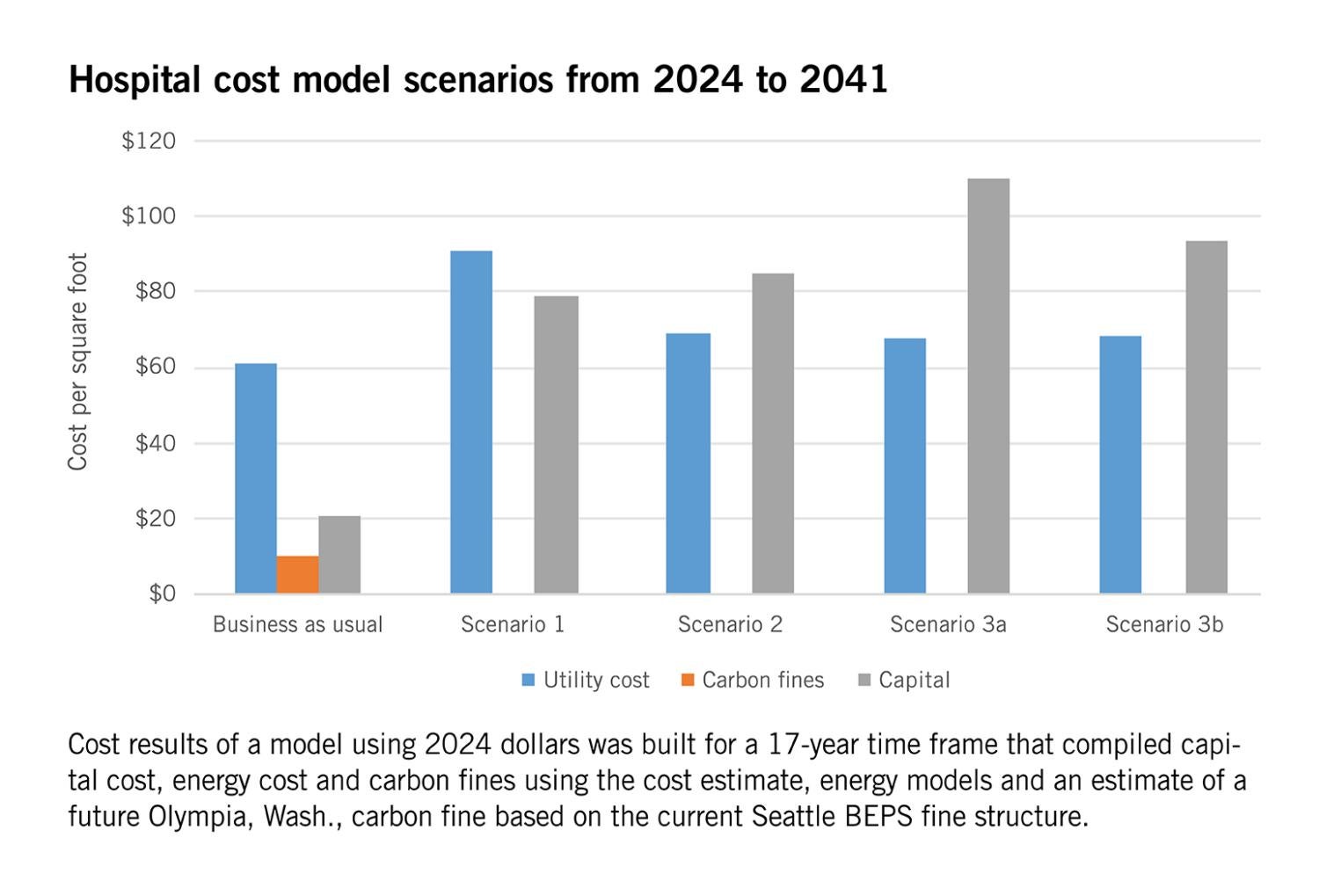
A cost model using 2024 dollars was built for a 17-year time frame that compiled capital cost, energy cost and carbon fines using the cost estimate, energy models and an estimate of a future Olympia carbon fine based on the current Seattle BEPS fine structure.
The total cost of ownership over 17 years for each case is as follows:
- Scenario 0: $67.2 million ($92 per square foot).
- Scenario 1: $124.2 million ($169 per square foot).
- Scenario 2: $112.6 million ($154 per square foot).
- Scenario 3A: $130.0 million ($177 per square foot).
- Scenario 3B: $118.4 million ($162 per square foot).
The most cost-effective fully electrified solution is Scenario 2, though it is still $45 million more costly over 17 years than Scenario 0, the business-as-usual case. It is worth noting that this study does not include utility rate escalations or utility incentives. Furthermore, some of the capital equipment, such as heat pumps, may decline in cost as the market matures.
Key takeaways
The research for the case study took place over a year, and several key takeaways were identified.
First, it is technically feasible for PSPH to decarbonize the thermal load. However, due to the nature of the hospital as a patient care environment and the need for normal operations, it will take 10 to 15 years to achieve carbon neutrality for the thermal load. This demonstrates the need for careful planning and early preparation.
Second, it is financially feasible for PSPH to decarbonize the thermal load. The study estimated that full electrification of the thermal load would cost around $100 per square foot in capital expenditures. Several financial mechanisms are available today that might help PSPH move forward with electrification, such as the incentives in the Inflation Reduction Act of 2022.
Finally, it is noteworthy that technologies for decarbonization are emerging and continually changing quickly. Equipment that is on the cutting edge today will be out of circulation by the time the thermal system is fully electrified. This emphasizes the need to plan early and be mindful that technologies will shift.
The study is not intended to be a playbook for electrifying any given hospital, nor is it meant to be a benchmark by which other hospitals pursuing this goal should be measured. The path to electrification is extremely complex. Each electrification plan must be tailored to the specific goals of a health care facility or system as well as the regulatory requirements that govern that facility and the needs of the communities it serves.
Related article //Goal and scope of the study
The goal of the study profiled in the accompanying main article is to determine the technical and financial feasibility of eliminating the hospital’s natural gas supply. The natural gas supply must be fully eliminated to achieve the project’s goal because the carbon emissions are tied both to the combustion of natural gas and the methane emissions associated with the upstream distribution of natural gas.
Ideally, the heating supply will fully eliminate fossil fuels, including on-site diesel fuel storage. However, this is a short-term stretch goal due to certain technologies, such as microgrids, not being mature enough yet.
The study focused primarily on Scope 1 carbon emissions related to combustion at the steam plant and the approaches required to electrify this system. Several systems were investigated, including the heating hot water supply systems, air distribution systems and terminal devices, along with the factors that drive the thermal demand, such as envelope performance, conditioning outside air and process loads. A secondary goal was a comprehensive energy assessment that included electricity, which is tied to Scope 2 emissions.
Fully characterizing the electrical system is critical to confirm that conversion of the natural gas heating load can be supported by existing electrical infrastructure to achieve beneficial electrification. The study was informed based on four key data sources: utility bills, collected building automation system data, performance testing and a calibrated energy model with supporting studies.
Details of each analysis are provided in the publication.
About the case study publication
The Electrifying Heat in an Existing Hospital: Providence St. Peter Hospital Decarbonization Case Study publication is a groundbreaking analysis conducted in partnership between the American Society for Health Care Engineering (ASHE) and Providence St. Peter Hospital in Olympia, Wash., that establishes the feasibility of electrifying the existing hospital building’s thermal load.
Prepared for ASHE by consultant Fred Betz, Ph.D., LEED AP, the study shows it is technically feasible to electrify the Providence St. Peter Hospital building’s thermal load; it is financially feasible to electrify Providence St. Peter Hospital’s existing building; and full decarbonization includes factors beyond the thermal load. It is organized into the following chapters:
- Chapter 1 provides an introduction.
- Chapter 2 contains the summarized results of all the studies that inform the decarbonization conclusions.
- Chapter 3 is a detailed description of the existing facility that forms the basis of the analysis.
- Chapter 4 describes experiments conducted on the hospital’s heating plant.
- Chapter 5 contains all the decarbonization studies that support the results section.
- Chapter 6 focuses on resilience aspects of the decarbonization study.
- Chapter 7 compiles a summary of the capital improvements needed to achieve decarbonization.
- Chapter 8 discusses construction phasing requirements to implement decarbonization in a functioning hospital.
The publication also features appendices with additional data, calculations and results that support the study.
This article was excerpted and edited by Health Facilities Management staff from the 180-page report Electrifying Heat in an Existing Hospital: Providence St. Peter Hospital Decarbonization Case Study.
Related Articles

NFPA weekly update: April 7-11
The NFPA 70 committee passed a tentative interim amendment on listing requirements for medium voltage cables and other components.

Equipped to meet sustainability goals
Hitting targets in energy savings requires having the right people and using the right technology.

NFPA weekly update: March 31 to April 4
Committees voted on revisions regarding preservation of physical records and practices in oxygen-rich environments.