
Capital investments for organizational efficiency

A multidisciplinary capital renewal committee should develop a prioritization method that considers multiple risk factors.
Image by Getty Images
Health care organizations rely heavily on their facility portfolio for the delivery of care as well as non-clinical functions that support the business of health care. The complexity and sophistication of these facilities continues to increase. These buildings will continue to be a necessary part of the health care landscape — even as they continue to age.
Allocating capital funding to maintenance projects is a continual challenge for facilities managers and their leaders. Programs intended to address capital needs vary from remedial spreadsheets to sophisticated systems and often use outside consultants and contractors. Because these projects are focused on sustaining the facility rather than adding new functionality, their return on investment is difficult to express and comparisons with other projects are not easily made.
This article was excerpted and edited from the American Society for Health Care Engineering (ASHE) monograph “Capital Renewal Playbook.”
Optimizing buildings
The purpose of a capital renewal program is to optimize the condition of a health care organization’s buildings, their functional life and available financial resources. This occurs through proactive identification of deficient conditions, effective capital budgeting and maintenance management based on accurate, objective data. The goal of ASHE for a capital renewal program ultimately aims to eliminate deficient conditions within buildings, thus sustaining the total functionality of the facility. In addition to natural deterioration, assessments may uncover code issues that could or should be addressed.
Essentially, assets are defined as any physical structure that can be assessed. Systems are components of an asset, such as roofing, HVAC, lighting, stairs, plumbing or electrical. Requirements are defined as deficient conditions that should be addressed, usually associated with a specific facility system.
If these maintenance requirements are not addressed, the condition of these systems continues to deteriorate, and the total of deferred maintenance requirements continues to mount. The effect of these deferred maintenance requirements results in an increase in the facility condition index (FCI)
To deal with deteriorating facility conditions, it is necessary to establish assessment programs to make accurate predictions and effectively replace systems prior to their failure. Maintenance and repair programs ensure that the lifetime of systems is optimized with proper maintenance; such programs require proper financing to ensure allocation of funds for system repair and maintenance. The total business response must be as timely and accurate as possible, relative to the actual facility condition need.
The absence of capital renewal programs will result in alternative methods of maintaining the asset. While these alternative systems may resolve issues, they are not proactive, can generally be unpredictable and often result in inefficient allocation of resources across the asset life cycle. Four dimensions of error can be used to describe the yield of such nonstrategic approaches: too much money, too little money, too early or too late (see below).
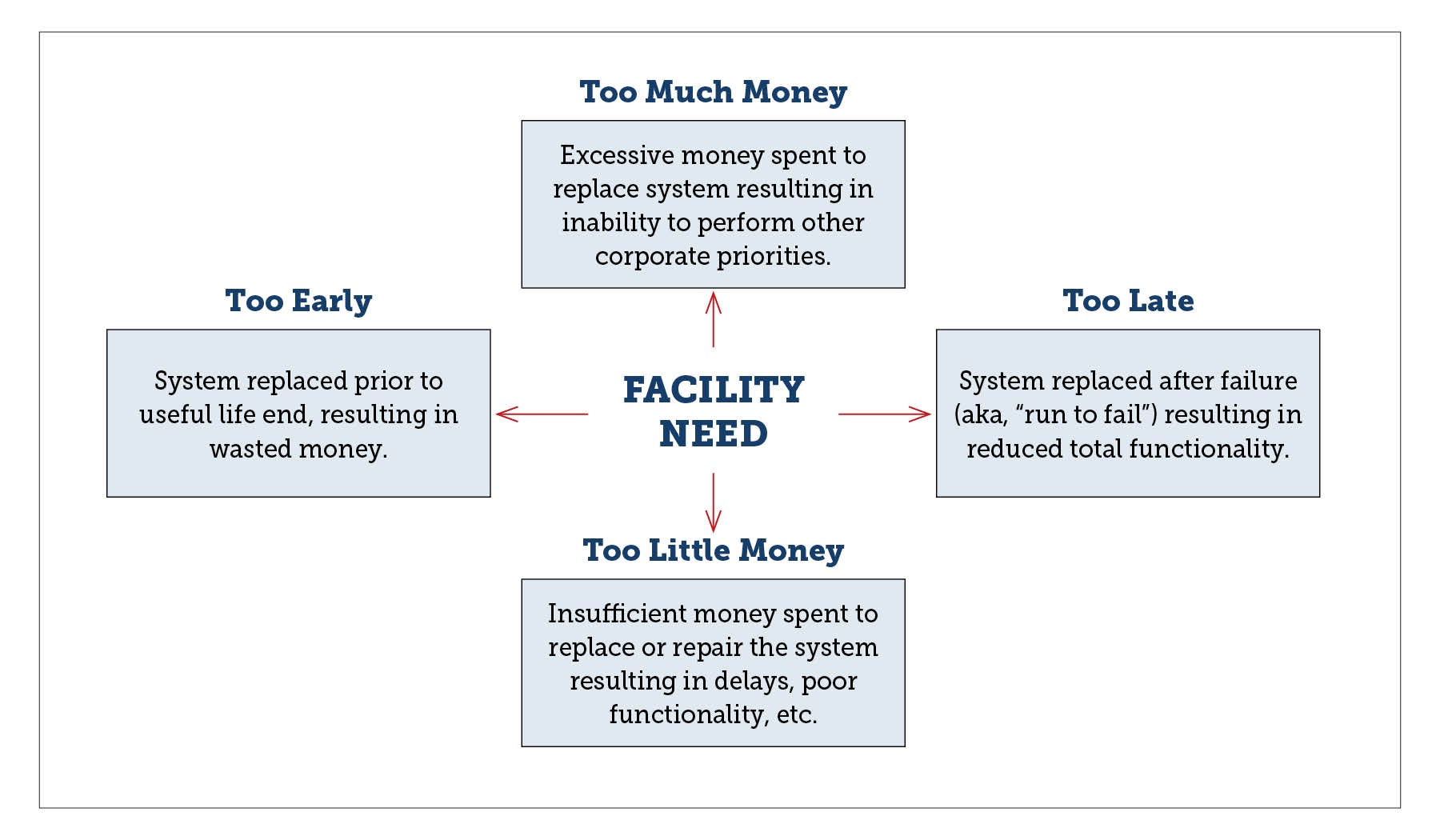
Click image to enlarge and for caption.
Because of these investment errors, on an aggregate level the portfolio will not be sustained. The implications of an increased backlog driving increased facility risk include direct, unscheduled operational effects, increased future maintenance cost and shortened facility useful and functional life.
Key elements
ASHE’s Health Care Executive Leadership Council conducted a study of successful capital renewal programs in large health care facility portfolios. The study identified the following 12 key elements of a successful capital renewal program:
Facility inventory. Facility inventory can be as basic or sophisticated as the organization requires. All buildings should be included in the inventory as individual properties. New buildings should have their information entered into the database on acquisition or completion of construction. This information will provide a baseline for future planning. In addition to information such as size, geographic location, number of floors, age and building type, the system should provide a means to track maintenance requirements from the time they’re identified until the time that they are addressed. Building data should be kept until facilities are formally decommissioned or disposed of.
Consideration should also be given to leased properties. In some cases, the tenant improvements that are funded by the health care organization remain their responsibility to maintain.
Often, health care organizations maintain similar databases for their computerized maintenance management system, master planning, real estate management, and capital planning and financial reporting. A thorough exploration of the need, feasibility, cost and value of enhancing or integrating these databases to meet the needs of the capital renewal program should be conducted. Accurate identification of potential failures in advance, as well as timely elimination of the deficient condition, is necessary to maintain and improve facility conditions and achieve the program targets.
Facility condition assessment. The facility condition assessment is the collection of detailed facility data derived from a systematic assessment process. The process supports a capital renewal program by identifying, estimating and prioritizing both existing deferred and anticipated major building systems’ capital renewal requirements. The assessment promotes facility functionality, which will deteriorate if an effective assessment and capital plan are not in place to address requirements in a timely manner.
For leased buildings, organizations are recommended to survey only what they are responsible for based on the lease. Prior to the survey, the organization should examine the lease and highlight systems under its responsibility on survey systems checklists. Facilities managers should pay particular attention to tenant improvements that have been funded by the organization; these should be surveyed as if they were an organizationally owned asset.
The assessment team should walk around the boundaries of the area for which the organization is physically responsible and identify any standards requirements for these systems as well as the age, lifetime and observed years remaining for each system they’re responsible for. An overview of the general building condition should also be provided. Replacement values for leased buildings may be calculated in the same manner as for owned buildings.
When a third-party facility condition assessment contractor or consultant is engaged, a tightly integrated partnership should be established. To help these contractors and the health care organization manage quality and quantity of work, both organizations should aim to do the following:
- Provide visibility to the long-term survey schedule.
- Aim to use a standard auditing team.
- Develop a survey schedule.
Metrics. The capital renewal program tracks facility condition using several metrics. Although this playbook provides additional metrics, the FCI is most often used for health care. Given that many factors influence these metrics (e.g., geographical and demand-based differences in market costs for repairs and subjective assessments of when repairs should be made), caution should be exercised when making comparisons among different organizations. These metrics are recommended to serve as internal references over time and not compared across facilities from different organizations. Facility condition metrics are all based on the cost and timing of maintenance requirements relative to the current replacement value of the facility.
- FCI (all current year and past due). This ratio is the sum of any “deferred capital replacement projects,” and the “current capital replacement projects” compared to the “replacement costs” of the same asset.
The method of calculating the replacement cost of the asset has a dramatic impact on the FCI. Therefore, the FCI is not an absolute and direct indication of condition; it serves as a useful index. In general, the lower the FCI, the better the current facility condition. In practice, most consultants and health care facility leaders agree that buildings with critical functions (e.g., hospitals and surgicenters) should aim for FCIs of .05. For other, less critical buildings (e.g., outpatient clinics and administrative offices) the FCI target is closer to .10.
An FCI of .15 means the deferred maintenance costs equal 15% of the cost of totally replacing the facility. For these facilities, systems and components — such as panels, pipes and wiring, as well as patient care systems like medical gas — may be as out of date as the physical structure (making it nearly impossible to find replacement parts because they are often no longer available). At the least, systems with medium-to-long life expectancies such as mechanical, vertical transportation and roofing have exceeded their useful life.
- Projected requirement index (PRI) (four years in the future). The PRI measures the “anticipated capital replacement projects” expected for a given number of years into the future in each building or group of buildings compared to the “replacement costs” of the same asset or assets. Generally, the higher the PRI, the greater the potential benefit of considering replacement of the entire facility.
- Facility maintenance renewal index (FMRI) (current, past due, and four years in the future). The FMRI is a composite metric to support capital replacement planning by providing a comprehensive view of both deferred and anticipated capital replacement project needs. Mathematically, FCI + PRI = FMRI. Generally, the lower the FMRI, the better the current and near-future condition of the facility. FMRI tends to smooth out aberrations in capital allocations over time.
- Sustainment percentage (based on a 10-year planning window). The sustainment percentage is an indication of the average percentage of current replacement value necessary to sustain the asset’s current condition each year within a 10-year planning window.
- Age of plant (AoP). The AoP is not a direct measure of physical age; rather, it is a financial ratio that measures how well a hospital is keeping its facilities up to date. The ratio is calculated as accumulated depreciation over depreciation expense. This AoP metric is reported across several facilities, and its median (to correct for extreme outliers) is published. The resulting median AoP score allows an understanding of the general state of the hospital infrastructure for any given period and allows for pattern tracking across years.
As the organization considers the use and interpretations of metrics related to the capital renewal program, timing of the overall capital cycle should be considered. This cycle includes identification of requirements, estimating, capital allocation, design, construction and commissioning. In many health care organizations, this can easily require two years or longer.
Alignment with organization vision, mission and strategy. As with any effective program, a capital renewal program should align with the organization’s vision, mission and strategy. Key shifts in health care delivery trends often have major effects on the use of facilities in the organization’s portfolio. An understanding of growth and expansion strategies will help guide decisions about capital allocations to the legacy portfolio. Decisions regarding new construction, mergers or acquisitions should be informed by a forecast of their potential effect on the capital renewal (and operational maintenance) program across the assets’ life cycle.
Integration with other strategies. Other organizational strategies can often support or be supported by a capital renewal program. For instance, brand image strategies can be supported by capital improvements to building facades and interior aesthetic elements. Likewise, energy strategies often benefit from investing in the most energy-efficient technologies available when considering the replacement of large energy-consuming devices or systems (e.g., lighting, heating and cooling). Additionally, information technology (IT) strategies are dependent on proper cabling, pathways, cooling and power. In addition to proactive replacement of aging systems, a capital renewal program can provide baseline funding that only requires augmentation to meet the growing IT footprint.
Efforts to improve the resiliency of buildings and building systems present another example of the synergy that can result from alignment of strategic initiatives. In some cases, augmented scope and funding of a capital maintenance project make resiliency projects more affordable.
Funding allocated specifically for capital maintenance. When a capital renewal program competes for funding in the same manner and at the same time that new investments in equipment and facilities are considered, capital renewal projects will have a more difficult time receiving priority, and high-risk maintenance projects may be deferred and funding allocated to other uses.
Over time, deferred maintenance can increase to a level that may be difficult to fund. Aging systems may enter actual failure modes, resulting in significant clinical and business effects. Research into successful capital renewal programs reveals that capital maintenance allocations are forecasted prior to most other allocations.
This high-level allocation often considers the sustainment percentage for the organization as a whole. This practice levels the playing field for capital decision-making: new projects and equipment aren’t directly competing for the funds required for sustaining the portfolio.
Agreed-on targets, goals and/or outcomes. A multidisciplinary capital renewal committee should work with the health care organization’s leaders to administer the program and to set targets. Targets should be based on building type with each having its own goal. The capital renewal program should help the organization not only achieve the targets, but should also aim to develop a maintenance strategy that applies capital “just in time.” Just as it is not appropriate to delay maintenance requirements that are due, it is equally inappropriate to replace systems much earlier than necessary.
Risk assessment/prioritization scheme. The capital renewal question most often asked by health care executives is, “What happens if we don’t do this?” For each maintenance project, there are multiple dimensions of risk, including:
- Technical. What is the likelihood that deferring this project will result in other related equipment or system failures?
- Operational. Will the failure of this capital maintenance requirement have a significant effect on operations?
- Clinical. Could the failure of a system from deferred maintenance bring about negative patient outcomes?
- Mission. Would the organization’s reputation be harmed by a system failure?
A multidisciplinary capital renewal committee should develop a prioritization method that considers multiple risk factors. While metrics associated with the management of a capital renewal program may be used to gauge the relative condition of a facility, they are not necessarily indicators of risk.
Multi-year assessment. Continual refreshing of maintenance requirements is necessary to keep program data current. Organizations may opt to perform surveys of the entire portfolio every three to five years. Some organizations provide a rolling assessment program, surveying a portion (20%) of the gross square footage of facilities each year.
Multidisciplinary team. In some health care organizations, the capital renewal program is managed and executed solely by the facility department. This approach has disadvantages:
- Decisions will not consider the organization’s goals as a whole.
- Opportunities for leveraging other department or division strategies will be lost.
- Support from other departments will be limited or nonexistent.
- Decisions, goals, targets and standards for the program will not have the support across the organization that is necessary for success.
A multidisciplinary approach is necessary for the implementation, management and improvement of a capital renewal program. While the actual composition of a capital renewal committee may vary given the size, structure and governance of the organization, representation should be considered from facility operations and maintenance, design and construction, energy management, financial planning, IT, security, biomedical engineering, infection control, environmental health and safety, strategic planning, risk management and leadership (executive sponsor).
Once formed, this group should be chartered to recommend and/or approve program structure, facility condition assessment program, metrics and targets, and risk assessment and prioritization. The group should meet periodically throughout the year to monitor, manage and revise the program as necessary.
Communications plan. In addition to providing communications to leadership, the communications plan should inform the organization. An awareness that a planned and proactive capital renewal program is underway sends a strong message to employees about the importance of facilities, encourages them to be good stewards of the asset and often causes them to be more receptive about minor business disruptions that might result from these planned projects.
Monitoring. At each meeting, the capital renewal committee should monitor the program’s progress. In addition to program metrics, it should also review the status of projects. Often, emergent situations will require reprioritizing or revising the project plan. The committee should also ensure that goals, objectives and incentives are aligned in a way that encourages and recognizes a program’s success. Each functional area represented on the capital renewal committee should be reviewed to determine whether goals specific to the program outcomes should be included in their performance plans.
A powerful tool
A comprehensive program of facility condition assessments and thoughtful forecasting of identified capital renewal requirements will provide the organization with a powerful strategic tool.
When aligned with the organization’s mission and other departmental strategies, these capital renewal programs avoid costly interruptions in health care delivery and manage costs over the life cycle of the assets.
About the ASHE monograph
This article was excerpted and edited from the American Society for Health Care Engineering (ASHE) monograph “Capital Renewal Playbook,” which was prepared by the ASHE Health Care Executive Leadership Council.
The authors were:
- Jonathan J. Flannery, MHSA, CHFM, FASHE, FACHE, senior associate director of advocacy at ASHE.
- Ramé Hemstreet, vice president of operations and chief sustainable resources officer, Kaiser Permanente.
- Gerry Kaiser, senior director of the facilities resource group at Ascension Health.
- Don King, CHFM, president of Donald King Consulting.
- Spencer Moore, MBA, MS, vice president of facilities management at University of Texas M.D. Anderson Cancer Center.
The sidebar "Creating a reliable renewal program" was written separately for this article.
A copy of the full monograph can be accessed by health care facilities professionals at ASHE's website.
Related Articles

The big change in annual incentive bonuses
More facilities professionals report bonuses being tied to clinical performance and patient safety goals.

NFPA weekly update: March 9-13
NFPA seeks public comments on new tentative interim amendment for weapons detection systems.

ACHC receives deeming authority extension for critical access hospitals
CMS recently granted the accrediting organization a six-year extension of deeming authority of critical access hospitals.