
Planning for future editions of NFPA 101

Fire and smoke barriers should be clearly identified.
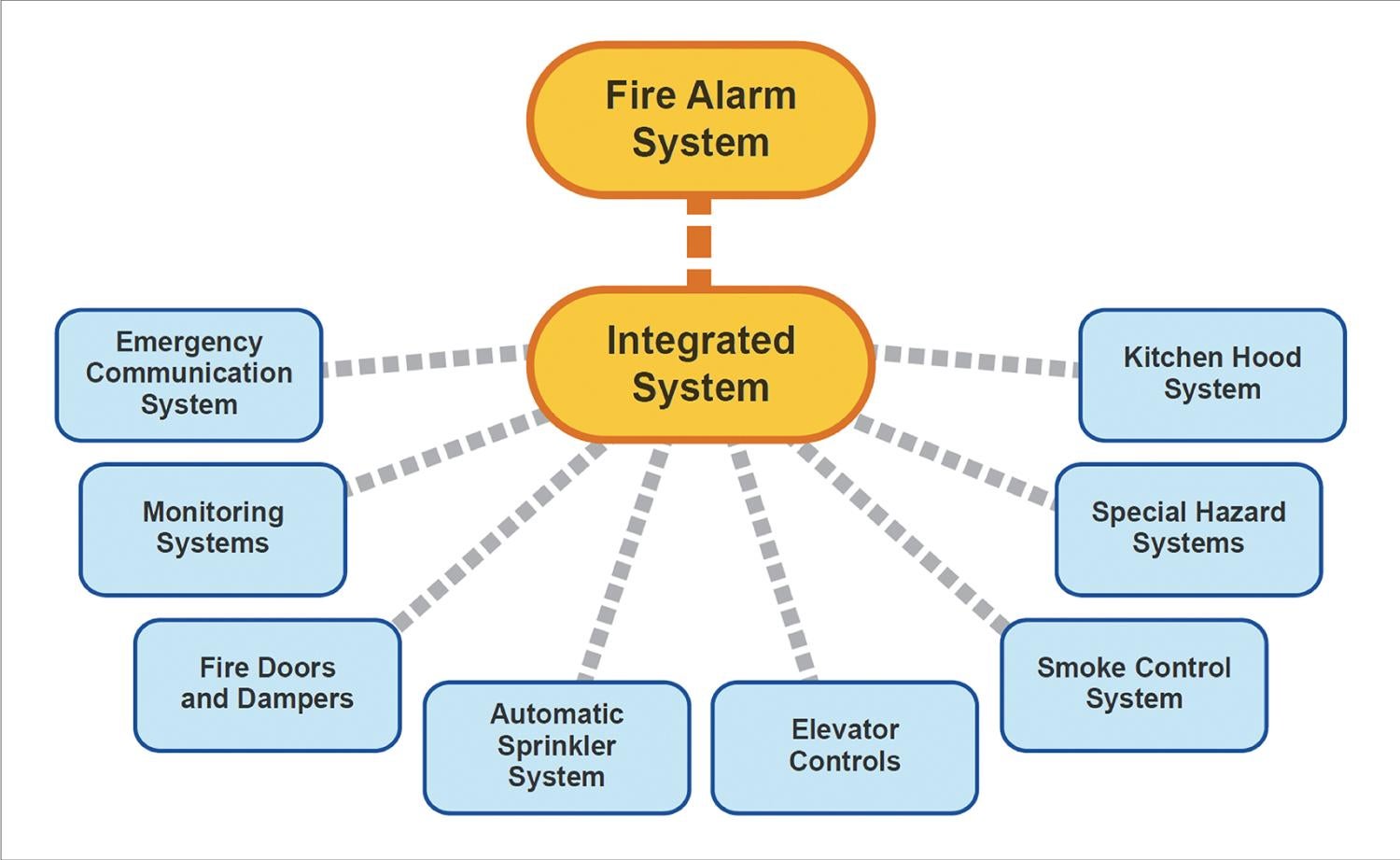
Image courtesy of Koffel Associates Inc.
The Centers for Medicare & Medicaid Services (CMS) continues to require compliance with the 2012 edition of the National Fire Protection Association’s NFPA 101®, Life Safety Code®, as one of its Conditions of Participation.
However, this article addresses the significant changes between the 2012 and 2024 editions of NFPA 101 and the challenges they may present. While it is not certain if or when CMS will adopt NFPA 101-2024, it is likely that CMS will eventually adopt it or a later edition. (The same holds true for NFPA 99, Health Care Facilities Code.)
By being aware of the significant differences in subsequent editions of NFPA 101 and managing their potential ramifications, design professionals and health care organizations can factor the changes into current and future projects.
Reference standards
When CMS adopts a more recent edition of NFPA 101, the reference standards will also be updated to the more current edition. However, upgrades to existing systems are not required at that time unless the authority having jurisdiction determines that the lack of compliance with the newer edition represents an unacceptable risk (NFPA 101-2024; 2.1(3)).
For instance, the provisions in the newer editions of NFPA 80, Standard for Fire Doors and Other Opening Protectives, and NFPA 105, Standard for Smoke Door Assemblies and Other Opening Protectives, regarding remote inspection dampers are probably among the more significant changes to consider. (They are discussed later.)
NFPA 80 also has a change regarding the inspection of fire doors. When the fire door inspection was first imposed on health care organizations through the adoption of NFPA 101-2012, many of those inspections were done based on a more recent edition of NFPA 80. To address that inspection issue more explicitly as it relates to fire doors, NFPA 80 now contains an annex note that indicates existing fire doors are to be inspected to the applicable code requirements at the time the door was installed (NFPA 80-2022; A.5.2.4).
Smoke compartments
Questions over various code editions also come up regarding smoke compartments. Surprisingly, some health care facilities are being designed today with smoke compartments up to 40,000 square feet, even though NFPA 101-2012 restricts the size of a smoke compartment to 22,500 square feet. Although recent editions of NFPA 101 and the International Building Code (IBC) permit certain hospital smoke compartments to be up to 40,000 square feet, using a maximum area of 40,000 square feet for a smoke compartment in a facility that intends to attain accreditation from CMS will be problematic.
As an alternative, a current design could take into consideration that CMS may allow smoke compartments up to 40,000 square feet in the future. For example, a facility could be designed based on 40,000-square-feet smoke compartments, including coordination with the fire alarm notification zones, by building “temporary” smoke compartments to achieve compliance with the current 22,550-square-foot limit.
When a subsequent edition of NFPA 101 is adopted by CMS, and if that edition allows smoke compartments up to 40,000 square feet, the temporary smoke compartments could be decommissioned. This would result in a reduced cost associated with maintaining smoke barriers that are no longer required and eliminating the cost associated with reconfiguring the fire alarm system to be consistent with the new smoke compartment configuration.
Another example of utilizing provisions in more recent editions of NFPA 101 during current projects would be to install fire, smoke and combination fire-smoke dampers that are capable of remote inspection and testing. The 2010 editions of NFPA 80 and NFPA 105 are silent on the issue of remote inspection dampers. However, the 2019 editions of NFPA 80 and NFPA 105 specifically allow the use of remote inspection dampers in lieu of the inspection and test requiring one to access and visually observe the damper.
Probably one of the more disruptive inspection, testing and maintenance (ITM) procedures is the testing of dampers, which typically requires access above ceilings serving as an infection control barrier and then a disruption of airflow for a period of time. Facilities managers may install remote inspection dampers along with the appropriate fire alarm monitor modules so a facility can change over to remote inspection and testing of the dampers when they are allowed.
Other ITM changes that should be noted include:
- Marking fire and smoke barriers. For several editions, the IBC has required that certain passive fire protection assemblies require a marking above the ceiling identifying the purpose of the barrier. NFPA 101-2024 has a similar requirement for new construction (8.2.2.5).
- Maintaining non-required fire doors. If a fire door is no longer required to be a fire door because the wall assembly is no longer required to have a fire-resistance rating, the door is no longer required to be maintained in accordance with NFPA 80 (NFPA 101-2024; 4.6.12.4).
- Inspecting exit signs. The requirement to perform an inspection of exit signs at intervals not to exceed 30 days (NFPA 101-2012; 7.10.9.1) has been deleted. There is still a requirement to test exit signs with a battery-operated emergency illumination source (NFPA 101-2024; 7.10.9).
Design considerations
The two most impactful changes with respect to the overall design of health care facilities are increased areas for nonsleeping patient care suites and smoke compartments.
With respect to suites, the 2012 edition permitted an increase in sleeping suites from 5,000 square feet to 7,500 square feet or 10,000 square feet, depending on how open the area is, the type of sprinkler installed and the presence of automatic smoke detection.
In developing the 2015 edition, it was noted that similar increases were not provided for nonsleeping patient care suites. With the 2024 edition, the area of treatment suites can now be increased to 12,500 square feet or 15,000 square feet, depending on how open the area is, the type of sprinkler installed and the presence of automatic smoke detection (NFPA 101-2024; 18/19.2.5.7.3.2).
However, the travel distance to an exit access door or a horizontal exit door is still restricted to 100 feet. The specific allowance to measure that travel distance to a horizontal exit is also a change from the 2012 edition (NFPA 101-2024: 18/19.2.5.7.2.4(A)).
With respect to the previously discussed hospital smoke compartments, the maximum area has been increased to 40,000 square feet, where all patient sleeping rooms are single patient rooms or suites and the smoke compartment is protected with fast-response sprinklers (NFPA 101-2024: 18/19.3.7.1). As with the suite provisions, the critical requirement of the maximum travel distance, in this case to a smoke barrier door, has been maintained at 200 feet.
Although the three-level communication space option (NFPA 101-2024; 8.6.6) is still not permitted in health care occupancies, they are becoming popular in certain areas of health care facilities. These spaces are permitted in business occupancies. Consequently, if the main entrance to the hospital is considered a separated business occupancy, the communicating space can be used there. Historically, one of the challenging requirements to meet is that the space is so open and unobstructed that a fire in any part of the space will become readily apparent to all occupants within the space. In lieu of meeting the “readily apparent” requirement, automatic smoke detection can be installed in the space (NFPA 101-2024: 8.6.6 (3)(b)).
Sterile cores supporting operating rooms and anesthetizing areas have been determined by several authorities having jurisdiction to be a hazardous area containing combustible storage in excess of 100 square feet. (This contrasts with a statement by the NFPA’s Healthcare Interpretations Task Force, which responded to a question during a June 2022 meeting about sterile core areas by saying that the area need not be protected as a hazardous area.) As such, the doors to these spaces need to be self-latching fire doors. New language in the 2024 edition of NFPA 101 specifically addresses the sterile core area and no longer requires the walls to be fire barriers or the doors to be provided with latching devices (NFPA 101-2024; 18/19.3.2.1.3(3)).
NFPA 101-2012 included provisions that addressed the vertical continuity of smoke barriers on floors other than health care floors. The challenge was that the floor below the health care occupancy was still required to have a smoke barrier unless it was separated with a floor assembly having a 2-hour fire resistance rating and if that floor was only used for mechanical equipment.
A separate exception omitted smoke barriers from open-air parking structures but not enclosed parking structures directly underneath a health care occupancy (NFPA 101-2012; 18/19.3.7.2). The allowance to omit the smoke barrier on the story underneath the health care occupancy has been expanded to any story beneath the health care occupancy provided there is not a health care occupancy on that story (NFPA 101-2024; 18/19.3.7.2).
Behavioral health units. Designing behavioral health units requires special consideration beyond the locking of doors for the clinical needs of the care recipients. One of the challenges in the past has been the confusing information provided to the care recipients.
Egress doors are commonly marked as such and appear like other egress doors in the facility. But due to the clinical needs of the care recipients, the doors are often locked, which can confuse an occupant. In NFPA 101-2024, murals may be provided on such doors provided they do not impair the operation of the door and, if a fire door, the signage is within the restrictions permitted for signage on fire doors in NFPA 80 (NFPA 101 18/19.2.2.2.7).
In other areas of the facility where door locking is required for the special needs of certain patients, the code has been modified to allow a facility to designate the egress paths that serve such areas. The requirement to unlock the doors upon activation of the smoke detection system or sprinkler waterflow alarm now only needs to apply to egress doors from the smoke compartment of fire origin, egress doors from any adjacent smoke compartment and only those egress doors from other smoke compartments that lead to one of the required, designated exits (NFPA 101-2024; 18/19.2.2.2.5.4(3)). Previous editions of the code contained a broader requirement that all egress doors unlock even if not serving the egress path from the smoke compartment of fire origin.
Fire alarm systems
Research has shown that there are certain areas of a health care facility in which audible and visual notification appliances could adversely affect patient care (e.g., neonatal intensive care units). In the past, audible alarm notification appliances could be omitted from critical care areas, but visual alarm notification appliances were still required.
Click image to expand
Today, the fire alarm system in many health care occupancies uses private mode notification. When that is used, both the audible and visual alarm notification appliances are permitted to be omitted where patient care is adversely affected (NFPA 101-2024; 18/19.3.4.3.1(2)). One could argue that these alarm notification appliances could be omitted in the past where private mode notification was used, but it is not explicitly permitted.
Also related to fire alarm systems is a relatively new NFPA standard that addresses the testing of integrated fire protection and life safety systems. Both chapters 18 and 19 require compliance with some of the integrated system test requirements in Chapter 9. While this is not required by NFPA 101-2012, it should be noted that the requirements for existing systems would apply in an existing facility once the 2024 edition is adopted. There is a requirement that integrated systems in existing buildings be tested at intervals not exceeding 10 years or as determined by NFPA 4, Standard for Integrated Fire Protection and Life Safety System Testing (NFPA 101-2024; 9.11.4.2.2).
As an alternative frequency, NFPA 4 permits the commissioning plan for a new system to indicate the required periodic testing of integrated fire protection and life safety systems. Therefore, if a facility is currently upgrading or replacing an integrated system, it may be beneficial to address the frequency of periodic testing in the commissioning plan, especially if testing at a frequency other than every 10 years is appropriate.
Many more changes
This article does not identify all the changes between the 2012 and 2024 editions of NFPA 101. There are many more changes that will impact the operation of health care facilities, including changes regarding waste containers and alcohol-based hand rubs.
It should be noted that if CMS adopts NFPA 101-2024, the adoption may include modifications to the language contained in the 2024 edition. It should also be noted that this article only addresses the provisions in NFPA 101-2024 as issued and not as it may be adopted by CMS.
RELATED ARTICLE: Assessments to reduce ITM costs
Maintaining life safety features that are no longer required increases costs for inspection, testing and maintenance over the life of the building. Life safety assessments focused on comparing existing conditions to the minimum required building and life safety code requirements can provide insight into the current use of spaces and allow facilities to downgrade or decommission some life safety features.
Assessing the following items is a starting point to determine which existing life safety features must be maintained:
- Use and occupancy. Patient care spaces are often vacated and replaced with noninpatient services upon opening new units. Rather than maintaining the life safety features required for health care occupancy, a change of occupancy to the new use of the space can have less stringent requirements.
- Electrical/telecom rooms. These rooms are often constructed with a 1-hour fire-resistance rating when newer transformer equipment may not require such protection. Assessing the equipment in the room may permit downgrading the rating of the enclosure.
- Protection of hazardous areas. Rooms not originally constructed to the requirements of new hazardous areas can meet less stringent requirements of existing hazardous areas. This allows downgrading from 1-hour enclosures to protection by smoke partitions.
- Sprinkler protection. Sprinkler protection throughout a smoke compartment permits the existing ½-hour corridor rating to be reduced to smoke resistive. As high-rise buildings become fully sprinklered by July 2028, the ½-hour corridor ratings can be reduced as each smoke compartment is protected with sprinklers.
A comprehensive detailed analysis needs to be performed on the overarching building to determine which life safety features are required to be maintained.
Sidebar by Adam Graybeal, PE, project manager for Koffel Compliance, Columbia, Md.
William E. Koffel, PE, FSFPE, SASHE, is senior director of special projects at Koffel Associates Inc., Columbia, Md.
Related Articles

NFPA weekly update: March 2-6
The latest updates on codes and standards for sprinkler system installation, fire alarm and signaling devices, and emergency communication systems.

NFPA weekly update: Feb. 23-27
Codes and standards on fire doors, emergency power systems and building construction safety codes move to the next stage.

NFPA weekly update: Feb. 16-20
The 2027 editions of NFPA's Life Safety Code and Health Care Facilities Code are open for the motioning process.