
Health care facility electrical demand loads

The design requirements for hospital feeder and branch circuit loads and the load growth assumptions justifying spare capacity are being reexamined.
Image by Getty Images
Most of today’s hospital buildings are operating as multi-specialty care facilities that use complex electrical systems to deliver high-quality care.
Additionally, hospital facilities need electricity for daily operations of building systems such as lighting, security, fire alarm, egress, HVAC and other critical infrastructure components.
Not to be forgotten are all the technological advancements that are spurring a significant uptick in the number of connected fire and life safety systems used in health care facilities. Many of these systems are being utilized around the clock and consuming high levels of energy.
Health care organizations are operating with small margins. As a result, facilities managers are increasingly striving for better efficiencies — a challenge that calls for analyzing and balancing the safety, comfort and green features in a building.
With all the digital and technological advancements used today, health care facilities have become more data-rich. The influx of insights and metrics offered by this data can help facilities managers make informed decisions with overall operational efficiency in mind. Furthermore, health care facilities are known for being one of the greatest energy consumers in the U.S., so sound data can help hospitals take steps to implement energy efficiencies on-site.
Resources such as the American Society for Health Care Engineering’s (ASHE’s) Energy to Care Program (energytocare.org) have been following this trend for years and offer tools for facilities managers to access, monitor and analyze energy usage data and adjust as necessary.
In November 2019, the Fire Protection Research Foundation (FPRF), the research affiliate of the National Fire Protection Association (NFPA), hosted an Electrical Data Summit where attendees evaluated the role of data in the electrical world, including electrical codes and standards. It was acknowledged during this forum that validated data can significantly support the code development process and guide regulatory bodies.
Historic factors
The standard for electrical safety, NFPA 70, National Electrical Code® (NEC®), provides the design and installation criteria for electrical projects around the world, but the health care load requirements for receptacles in the NEC have seen few modifications since the 1970s.
Factors such as the use of more energy-efficient systems and the vacating of oversized equipment for more efficient cost-saving options are driving down the electrical load of end-use equipment. As a result, the design requirements for feeder and branch circuit loads and the load growth assumptions justifying spare capacity are being reexamined.
Although there is growing evidence to support the need to modify existing demand factors, the following historic assumptions have caused hesitation with updating health facility demand factors:
- Quantity and quality of data collection. A statistically significant amount of electrical load data is required to validate the appropriateness of demand factors for health care facilities. However, what constitutes a statistically significant sample size has been long debated.
Studies in the past have collected electrical load data for periods varying from a few weeks to a month. This short duration of data collection has faced resistance in the code-making process as it may not be representative of other influencing factors, such as seasonal influences on electrical demand in various geographic locations.
In different regions of the country, building construction and engineering design practices may differ due to climate, weather, local building regulations and energy conservation codes. To obtain an accurate representation of electrical load behavior and demand, many believe that electrical loads would need to be measured over the span of at least one year.
Determining the proper sizing of electrical equipment is also dependent on an accurate representation of the electrical loads when the facility is operating at full capacity. If readings are taken while a hospital is not at full capacity, the load readings may represent an inaccurate assessment of demand and lead to undersizing of equipment, posing a safety concern.
In hospital settings, all the connected loads are either connected to an essential or nonessential (normal) electrical system. Essential systems, including select life safety systems, critical branches and equipment branches, are vital for safe and effective facility operations. Essential life safety systems typically include those required for notification and safe egress: the critical branch serves critical patient care areas, fixed equipment and special units like blood banks, among others; and the equipment branch serves electrical equipment deemed essential for patient care and baseline health care facility operation.
Meanwhile, there are nonessential systems which don’t require backup power. General lighting, noncritical service equipment, general lab equipment and other systems fall into this category. However, there have been some concerns that past research studies did not address both branches of electrical systems in hospitals.
- Different electrical demands. It is a fair assumption that electrical demand may differ in different types of (or spaces within) health care facilities, potentially warranting distinct demand factors. The size of a facility, its geographic location and other variables also are believed to influence electrical demand.
Even within health care buildings, there are variables to consider. For example, an intensive care unit area may have a higher electrical load than a waiting room. Therefore, all department types should be measured over a long period of time to determine appropriate demand factors.
In the past, studies generally have measured loads at the branch circuit and panel levels. There have been misconceptions around how panel loads aggregate at higher levels of the distribution system. Due to the law of probabilities, the anticipated peak loads at higher levels of the system get lower than the aggregated sum of the underlying panel loads because all panels do not operate simultaneously at their peak loads. Therefore, application of a demand factor gives a more conservative result at higher levels of the distribution system.
- Spare capacity to meet a potential surge. The importance of measuring electrical load data when a hospital is operating at full capacity has been noted and has led some to argue against reducing spare electrical capacity in case it is needed for adverse events.
Some fear that more than 200% spare electrical capacity may be needed during a significant surge caused by an event like a pandemic. The argument is that the loads in a hospital would skyrocket and, unfortunately, readings taken during normal times would not accurately reflect the level of electrical demands witnessed during a potential surge.
It makes sense to plan for catastrophic events, but how much excessive spare capacity is appropriate for electrical system design considerations? It is believed the excess spare capacity may be beneficial in the case of potential health care facility expansion or renovation. However, current NEC provisions are intended to ensure that a safe electrical system is built but does not factor in future expansion of electrical use.
Research project
To address some of the feeder and branch circuit sizing questions, NFPA and ASHE sponsored a study conducted by FPRF titled, “Electric Circuit Data Collection: An Analysis of Health Care Facilities” (see the resource box on page 34).
The overarching goal of the study was to provide the NEC code-making panels with the most recent, relevant information on measured electrical receptacle load demands in health care facilities for the standards development process. The amount of validated, high-quality data that was captured as part of this project was intended to help NFPA code-making panels develop key guidance to make informed, data-driven decisions around potential code changes.
The timing of this project coincided with the COVID-19 pandemic, which severely burdened health care systems globally. During this period, many hospitals were operating at full capacity. Although pandemic situations are rare, they put the electrical load demand assumptions to the test when they occur. Conversely, during COVID-19, many hospitals canceled elective procedures in anticipation of a flood of COVID-19 patients. Not surprisingly, hospital occupancy fluctuated in concurrence with the surge and dip of COVID-19 cases and hospitalizations, as shown in Figure 1 below.
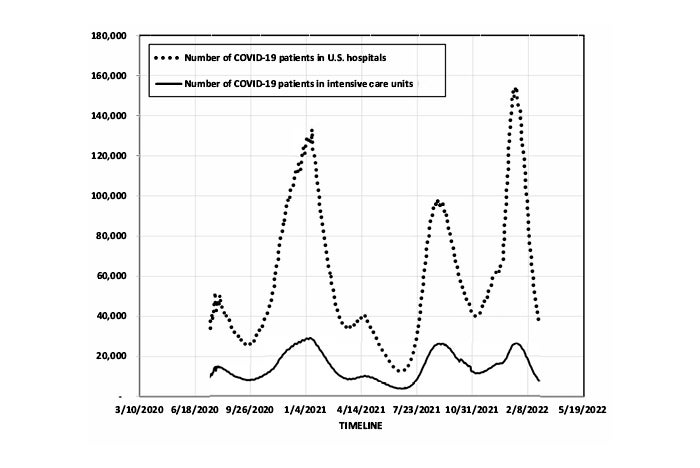
Figure 1. Occupancy of COVID-19 patients in U.S. hospitals (2020-2021).
Graphics courtesy of FPRF
The original scope of this study was not solely focused on health care facilities, but the pandemic presented an opportunity to gather pivotal data in response to some longstanding concerns from the NEC code-making panels. Included among them was the question, “What impact will a pandemic have on electrical systems?” Thus, the scope of research was modified to capture circuit and panel level receptacle data in patient care areas where surges were expected.
Implementation steps
The research project was led by Mazzetti, a mechanical, electrical and plumbing health care engineering, planning and design firm. The research team measured, collected and analyzed electrical load data in seven health care facilities, including community hospitals, urban hospitals and academic medical centers.
- Data quality and quantity. The data collection took over one year (between March 2020 and May 2021) and involved facilities located on the West Coast, and in the Southeast and Northeast regions of the United States.
The electrical load readings captured during the one-year period showed consistency among all the participating hospitals, despite the analysis being limited by the availability of metering equipment, hospital floor plans, electrical panel schedules and hospital census data. This indicates that one year of data may not be necessary to gauge the electrical demand of a facility.
Additionally, the data revealed that the geographic diversity and type of health care facility had minimal impact on electrical loads. These findings are consistent with the observations referenced in a prior study, “Plug and Process Loads in Medical Office Buildings,” that looked at outpatient facilities and touched on different demand factors in all health care facilities.
To address another historic concern of NEC code-making panels, the study captures electrical load data from all branches (both essential and nonessential panels) so that these areas of health care facilities were reflected in the analysis.
- Data insights. The data analysis highlighted that the current NEC demand factors for patient care areas in hospitals result in systems that are at least twice as large as needed for all the receptacle loads. The spare capacity increases at higher levels in the distribution system and is more significant for dedicated receptacles than for general receptacles.
These results are consistent across geographies and hospital sizes, ages and types, and did not vary over the study duration of one year. The study focused on peak loads over the measurement period and panel level analysis used sum-peak methodology to ensure that the results are reliable and conservative. The general and dedicated receptacle loads for hospitals did not appear to substantially increase during a pandemic.
- Impact of the pandemic. The electrical loads did not skyrocket as feared during COVID-19. This could largely be due to the way hospitals handled surge management in times of crisis — they canceled elective procedures, diverted patients to other sites, set up surge facilities and sometimes even had to turn away patients. This lessened the impact of surge on peak electrical demands. The limitations of other systems in the hospital such as staff and equipment also had an impact. Because health care systems are rate-limited, the data suggests that the potential benefit of excess electrical capacity for this purpose may be limited.
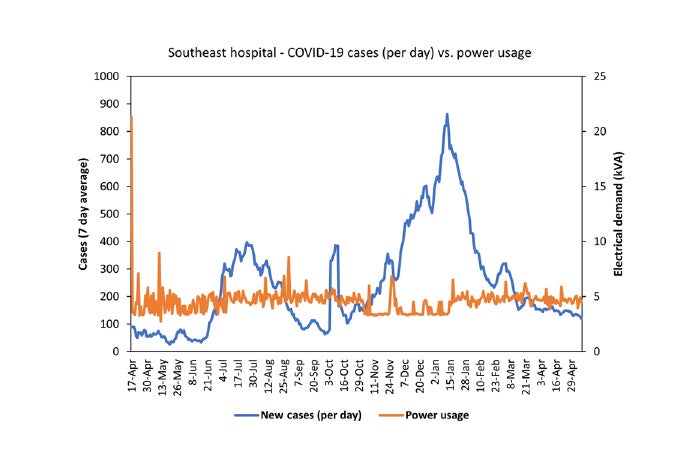
Figure 2. Daily COVID-19 cases versus power usage (April 2020-2021).
Graphics courtesy of FPRF
To correlate hospital electrical demand data with pandemic hospitalization surge factors, COVID-19 hospitalization data and/or county-level COVID-19 case rate numbers also were considered in the research analysis. Figures 2 (above) and 3 (below) highlight the consistency of the electrical loads over time despite rising COVID-19 cases and hospitalization rates in one representative hospital from the study.
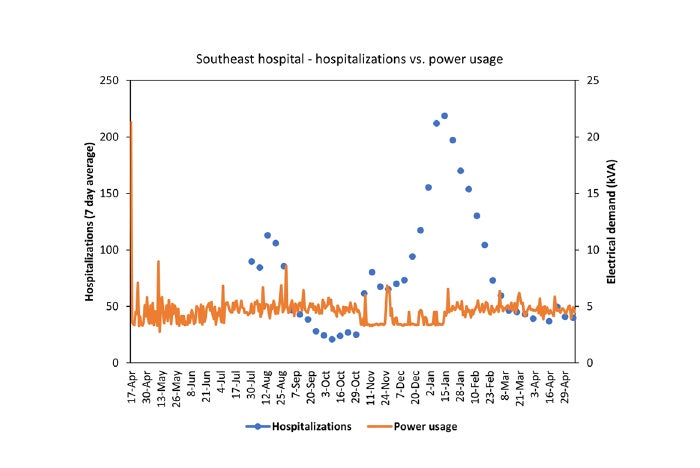
Figure 3. Hospitalizations versus power usage (April 2020-2021).
Graphics courtesy of FPRF
- Spare capacity. The data analysis of the spare capacity above the maximum measured load at the panel level varied between 111% and 1,198%. Although the study did not measure loads upstream from the branch circuit panels, the trends of increasing spare capacity at higher levels of the system from the cumulative effect of adding panels was clearly identified in the data, as shown in Figure 4 (below). The analysis found that the demand factors at higher levels of the system require even lower capacities than the demand factors for the branch circuit panels.
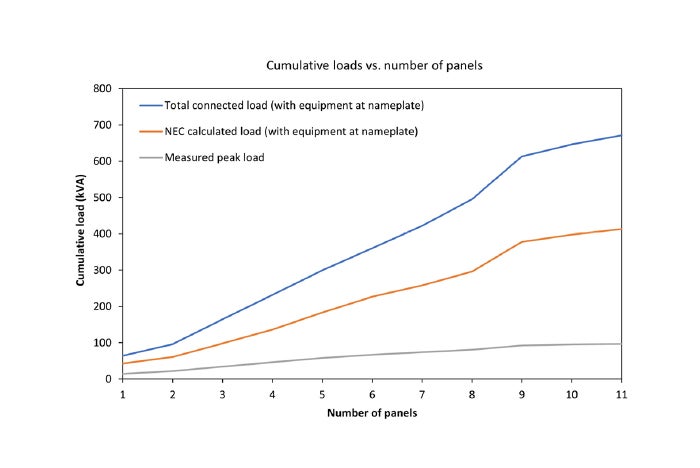
Figure 4. Cumulative loads versus number of panels.
Graphics courtesy of FPRF
Substantial data
During normal times and precarious moments in history, electrical engineers, facilities managers and code-making panelists are tasked with ensuring that electrical systems have sufficient capacity for both routine and emergency power demands.
The research project generated substantial data so that NEC code-making panels can reassess current NEC branch-circuit, feeder and service load calculations, particularly for receptacle loads. And potential changes to the demand factors reflected in the NEC are now in the hands of the volunteers who are part of the NFPA consensus codes and standards development process.
At the least, this new research will help foster more in-depth conversations about electrical loads in health care settings and will, ideally, lead to more discussion about energy conservation and sustainability in hospitals, clinics and specialty sites.
Data for safety and efficiency
Hospital facilities are unique and use complex electrical systems for their day-to-day operations that are required to maintain safe environments that are on par with competent health care.
The National Fire Protection Association’s NFPA 70, National Electrical Code® (NEC®), serves as the backbone of the regulatory and safety infrastructure for electrical systems.
Spare capacities are built into the electrical systems as a critical safety parameter to safeguard during an unanticipated surge of electrical load or for facility expansion. However, excessive spare capacity could also result in oversized equipment.
Striking this balance is critical for right-sizing electrical equipment. How much spare capacity is required to manage unprecedented surges in electrical demand (e.g., for a health care facility during a pandemic)? On the other hand, how much spare capacity is excessive while considering efficient design of electrical systems?
A comparison of electrical load data from both “normal” (i.e., pre-pandemic) and “surge” (i.e., during pandemic) operating conditions will provide needed insight on spare capacity provisions for future changes to codes and standards.
The Fire Protection Research Foundation recently published a research study titled, “Electric Circuit Data Collection: An Analysis of Health Care Facilities” (see the resource box on page 34), which captured electrical load data from seven hospitals across the U.S. over a one-year period during the COVID-19 pandemic. It was sponsored by NFPA and the American Society for Health Care Engineering.
The data obtained from a West Coast hospital during the pandemic showed spare capacity above the maximum measured load at electrical panels serving patient care areas varied between 199% and 1,198%. To contrast with pre-pandemic operating conditions, electrical load data collected from another West Coast hospital through a prior research study indicated a similar trend with spare capacity ranging from 163% to 1,171%.
These data revealed consistency among electrical demands during both “normal” and “surge” conditions, negating fears of severe fluctuations. The real-world data presented in this important project will enable future considerations of adjustments to the spare capacity requirements for hospital loading.
About this article
This feature was published by Health Facilities Management in partnership with The Fire Protection Research Foundation, the research affiliate of the National Fire Protection Association.
Victoria Hutchison is research project manager and Sreenivasan Ranganathan, Ph.D., is research director for The Fire Protection Research Foundation, the research affiliate of the National Fire Protection Association. They can be reached at vhutchison@nfpa.org and sranganathan@nfpa.org.
Important notice: Any opinion expressed in this article is the personal opinion of the authors and does not necessarily represent the official position of FPRF, NFPA or its technical committees. In addition, this piece is neither intended, nor should it be relied upon, to provide professional consultation or services.
Related Articles

NFPA weekly update: March 2-6
The latest updates on codes and standards for sprinkler system installation, fire alarm and signaling devices, and emergency communication systems.

NFPA weekly update: Feb. 23-27
Codes and standards on fire doors, emergency power systems and building construction safety codes move to the next stage.

NFPA weekly update: Feb. 16-20
The 2027 editions of NFPA's Life Safety Code and Health Care Facilities Code are open for the motioning process.